

Year: 2000 Vol. 66 Ed. 5 - (14º)
Artigos Originais
Pages: 512 to 518
The Use of Inspiratory Phonation t Characterize Laringeal Benign Lesions.
Author(s):
Milene V. Lopes*,
Mares Behalau**,
Osiris O. C. do Brasil***,
Deborah Andrade****.
Keywords: larynx, diagnosis, disphonia
Abstract:
Introduction: Inspiratory phonation is the voice produced during inspiration. Besides being a powerful therapeutic technique, this strategy was already used to help in the identification of laryngeal vestibule tumors. Aim: The goal of the present study is to verify the contribution of inspiratory phonation for clinical diagnosis of laryngeal benign mass lesions. Material and method: Thirty-one participated at this study, - with mass lesions and vocal complaints. Patients were asked to do both normal expiratory sustained phonation followed by an inspiratory one. Both images were taped and selected parameters were thus analyzed. Results: The main results indicated that inspiratory phonation have contributed to diagnosis in 90,32% of the cases. Inspiratory phonation has helped to define the mass lesion, particularly when vocal cysts were considered, leading to define the location of the lesion on the lamina propria. The more superficial the lesion, the larger mucosal expansion obtained, the better the vocal ligament visualization. The deeper the lesion, the smaller mucosal expansion and sometimes no vocal ligament visualization at all. Conclusion: Therefore, inspiratory phonation for diagnostic purposes contributes to characterize vocal fold cover mass lesions, enhancing the ability to localize the lesion and to establish the integrity of the mucosa through the vocal ligament visualization.
![]()
INTRODUCTION
Inspiratory, inhalation or reverse phonation is the production of voice during inspiration, that is, when air is coming into the lungs, exactly the opposite of regular phonation.
Timcke, Leden and Moore10 suggested that inspiratory speech is rarely present during conversation, but rather during laughs, cry and other emotional manifestations. They observed that during inspiratory phonation arytenoids are not totally close, forming a posterior triangle similar to what happens in whispered voice. As to aerodynamic principles, the authors differentiated inspiratory phonation from expiratory phonation by two main factors that complement each other: suction of Bernoulli's effect and closing effect produced by the anatomical configuration of vocal folds. Static air pressure above vocal folds during inspiratory phonation tends to force the folds one against the other. On the other hand, during expiratory phonation, subglottic pressure produces the opposite effect, that is, opening of vocal folds.
Inspiratory phonation is currently known and used especially due to its efficacy as therapeutic technique z, as compensatory phonation of some vocal and laryngeal alterations6, and it has already been used to support diagnosis of laryngeal vestibule tumors by radiological analysis7.
Even with the advent of optical fibers in laryngoscopic study what resulted in better visualization of larynx, otorhinolaryngologists frequently face difficulties in diagnosing lesions observed during the exam, be it through laryngeal telescope or nasofibroscope. Diagnosis of mass lesions is doubtful; inflammation, edema and contralateral reactions associated with the lesion may mask a primary lesion. The use of stroboscopy may be very helpful, as suggested in the literature3,1,8, however, unfortunately, it is not a resource available to all otorhinolaryngologists.
Therefore, the objective of the present study is to use inspiratory phonation during laryngeal exam of patients who have voice complaints and benign vocal fold pathologies and check its diagnostic contributions to identify and characterize these lesions.
MATERIAL AND METHOD
We examined 31 subjects who had mass lesions and vocal complaints and were in the age range of 23 to 52 years.
Subjects were submitted to laryngeal exam, carried out with rigid telescope brand Machida, model LCY-32.70°, microcamera brand Panasonic, system CCD, video model Sony, recorded in NTSC and speed SP on magnetic tapes brand TDK.
We employed topic anesthesia with xylocaine 10%. The exam was performed in two steps: first, conventionally, with expiratory phonation of vowels "e" and "i", at speech habitual frequency and intensity; next, the patient was instructed to carry out three consecutive inspiratory phonation maneuvers, that it to say, expire all air from the lungs, and inspire again producing the vowels "e" and "i", and sustaining them for some seconds.TABLE 1 - Numerical and percentage distribution of contribution of inspiratory phonation to otorhinolaryngologic diagnosis ( N = 31).
In a pilot study based on the analysis of the video and comparing both productions, we noticed that inspiratory phonation enabled visualization of structures that were not visible during expiratory phonation - we could see presence or absence of superficial layer of lamina propria and vocal ligament, more or less marked lesion and its location on the layers of lamina propria.
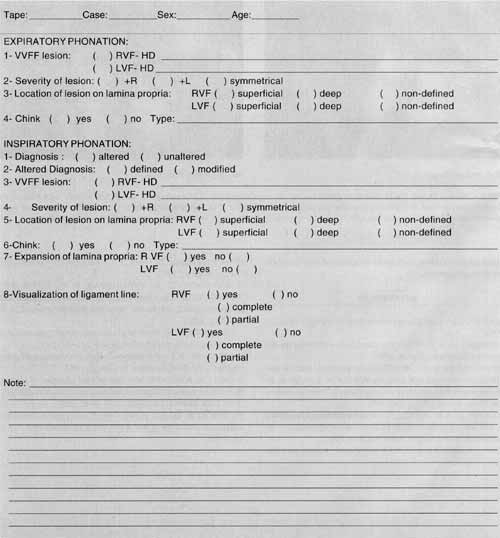
A protocol was created (Annex 1) to be filled in with data from both productions after visual analysis of recorded images. The protocol had common and complementary parameters to both phonations. The following parameters were analyzed: diagnostic hypothesis (considering type of identified lesion); definition of diagnosis (unaltered or altered diagnosis, and the latter was reclassified in defined or modified); location of lesions on mucosa layers (superficial, deep or non-defined lesion) and visualization of vocal ligament (complete, partial or absent).
RESULTS
The main results may be found in Tables 1 to 4. Table 1 presents contribution of inspiratory phonation to otorhinolaryngologic diagnosis, in which we pointed out the gain obtained from using this maneuver, both for definition and modification of initial diagnosis during conventional procedure.
Table 2 presents types of lesions found in both modes of phonation and we noticed that inspiratory phonation contributed to define the so-called vocal fold masses, highlighting the presence of cysts.
Table 3 shows the contribution of inspiratory phonation for location of lesion on superficial or deep layers of lamina propria, whereas Table 4 shows the visualization of vocal ligament in both productions.TABLE 2 - Types of lesions identified in expiratory and inspiratory phonation.
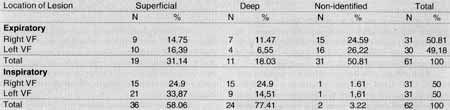
TABLE 3 - Location of lesion on lamina propria and right and left vocal folds (VF), in the two kinds of phonation.
TABELA 4 - Numerical and percentage distribution of the correlation between location of lesion and visualization of vocal ligament in inspiratory phonation.
COMMENTS
The use of inspiratory phonation during laryngeal exam proved to be a simple maneuver, easy to learn and to conduct by the patient, and with a high potential of improving diagnosis of the so-called mass lesions of the vocal folds.
Therefore, analyzing the contribution of inspiratory phonation in otorhinolaryngologic diagnosis, results showed that the procedure is very helpful, because in 90.32% of the cases the diagnosis was altered, and in only 9.67% there was no modification of initial diagnosis (Table 1). It was also observed that within modified diagnosis, 60.71% of cases had a better definition of lesions, that it, inspiratory phonation provided important data for definition of a previous hypothesis. In 39.28% there was total modification of diagnosis initially made based on-expiratory phonation, because some lesions could only be observed through inspiratory phonation. This is an unquestionable contribution, because speech and voice therapy is becoming more precise and relies more and more on data provided by laryngeal exam and vocal and acoustic analyses. Correct diagnosis leads to better treatment, shorter duration of therapy and minimizes treatment costs, delivering services of better quality to patients.
1A. Expiratory Phonation.
1B. Inspiratory Phonation.
CASE 1 - Photos 1A and 1B: In expiratory phonation, a poorly-defined irregularity on the middle 1/3 of right vocal fold is observed, and inspiratory phonation showed microcyst, located superficially on the lamina propria of right vocal fold.
As to types of lesions found in both modes of phonation (Table 2), we noticed that 11 cysts were diagnosed with inspiratory phonation and 10 mass lesions were better defined. Among diagnosed cysts, we observed in Case 1 that during expiratory phonation (Photo 1A) we could barely see a poorly defined irregularity, but during inspiratory phonation (Photo 1 B) a microcyst was diagnosed. Differentiation among nodules and cysts were not made, because the number of cases of nodules (two cases) was too small. However, the usefulness of the maneuver when diagnosing cysts, was unquestionable. In the same Table, it is interesting to observe that two sulcus diagnosed during inspiratory phonation were masked by existing inflammations and edemas, hindering visualization during conventional exam.
As to location of lesions on lamina propria (Table 3), out of 31 undefined lesions during expiratory phonation, 29 were defined after the performance of inspiratory phonation. We may conclude that this was the main contribution to diagnosis, since once we define location of lesion as superficial or deep, we may relate the various types of lesion, because the development of such alterations follows a very specific criteria on the different layers of lamina propria, as reported by some authors3,8. As to cysts, since they may manifest on superficial layer as well as firmly adhered to deep layers, the maneuver of inspiratory phonation is very useful when referring the patient, :making surgical decisions and defining therapeutic, pre and post-operative prognosis.
Gray, Hirano and Sato5 described the superficial layer of lamina propria as the most defined, loose and flexible during vibration, but it may be subject to toughening as a consequence of some type of inflammation, tumor or scaring. During inspiratory phonation, it was observed that more rigid lesions prevented a good expansion of superficial layer of lamina propria and, consequently, limited and hindered visualization of the line of vocal ligament (Case 2, Photos 2A and 2B and Case 3, Photos 3A and 3B).
The better vocal fold vibration is the better vocal quality. Sato and Hirano9 stated that the most important region for vibration pattern of vocal fold is the recovering layer, formed by epithelium and superficial layer of lamina propria, intermediary and deep layers. Thanks to the force of inspiratory phonation, it is possible to observe how these structures behave, what is not seen during conventional exam. It is noticed that if there is integrity of mucosa, we may observed by transparency the expansion of its superficial layer and exposure of vocal ligament - intermediary and deep layers. During inspiratory phonation, it is possible to observe detachment of superficial layer over the more internal layers. On the other hand, if there is mucosal rigidity, this effect tends to be absent, because the tissue is more rigid, as confirmed by Colton and Casper4.
2A. Expiratory Phonation
2B. Inspiratory Phonation.
CASE 2- Photos 2A and 2B: Expiratory phonation shows a lesion with polypoid aspect on the left vocal fold, suspect of the most important lesion, incomplete coaptation and double chink. Inspiratory phonation reveals lesion on left vocal fold corresponding to mixomatous collection located on lamina propria, without cicatricial processes, because there is its expansion and complete exposure of vocal ligament, presented uniformly. On the right vocal fold, it is noticed that there is no expansion of lamina propria, and vocal ligament is not individualized. Modulation of its middle third and presence of vascular dysgenesis are observed. This finding demonstrates that the mo important lesion is on the right vocal fold, and not on the left, as suspected based on expiratory phonation.
In Table 4, it may be observed that when the lesion is superficially located, visualization of vocal ligament is bettertotal in 86.1%, partial in 8.32% and absent in 5.54% of cases. If the lesion is on the deep layer, visualization of ligament is impaired, because in 50% of the cases it was not visualized, in 45.83% it was seen partially and in 4.16% it was totally visualized.
It was not possible to correlate type of lesion, expansion of lamina propria and visualization of vocal ligament, because not all lesions were classified into specific categories, and many of them remained only as mass lesions, mucosa irregularities or edemas. However, we could conclude that the smaller the compromise of lamina propria, the higher the likelihood of its expansion, and consequently, better vocal ligament exposure. In cases of edema, the larger they were, the larger was the expansion of superficial layer of visualized lamina propria. When lesions were more rigid, more adhered to internal layers, expansion of lamina propria and visualization of ligament were either reduced or absent.
Therefore, inspiratory phonation helps define more precisely the lesion as to location of lamina propria layers of vocal fold, leading to more defined diagnostic hypotheses. Differential diagnosis of nodules, polyps and cysts can not be performed in all situations, but the additional information provided helps support the diagnostic hypothesis.
CONCLUSION
Based on the use of inspiratory phonation in laryngoscopic assessment of patients with vocal complaints and presenting mass benign lesions of vocal folds, we concluded about inspiratory phonation that:
1. It added relevant information to diagnosis, defining, altering or revealing mass lesions;
2. It contributed to identify mass lesions and their specific characteristics;
3. It enabled localization of lesion in terms of vocal fold lamina propria layers; and
4. It demonstrated that when there is integrity of vocal fold lamina propria recover layer, there is expansion and visualization of vocal ligament.
3A. Expiratory Phonation.
3B. Inspiratory Phonation.
CASE 3 - Photos 3A and 3B: In expiratory phonation we observed irregularity of free margins of middle 1/3 on both vocal folds, more punctform on the right. Inspiratory phonation revealed normal expansion of lamina propria on the left, and perfect exposure of vocal ligament, presenting bowing. On the right vocal fold, there is no expansion of lamina propria, suggesting its impairment.
REFERENCES
1. ABITIBOL, J. - Atlas of laser voice surgery. San Diego, Singular, 1995.
2. BEHLAU, M. & PONTES, P. - Avaliação a tratamento das disfonias. São Paulo, Lovise, 1995.
3. BOUCHAYER, M. & CORNUT, G. - Instrumental microscopy of benign lesions of vocal folds. In: FORD, C.N. & BLESS M. D. Phonosurgery assessment of management of voice disorders. New York, Raven,1991. p.143-165.
4. COLTON, H. R. & CASPER. J. K.- Compreendendo os problemas de voz uma perspectiva fisiológica ao diagnóstico a ao tratamento. Porto Alegre, Artes Médicas, 1996.
5. GRAY, S.; HIRANO, M.; SATO, K. - Molecular a cellular structure of vocal fold tissue. In TITZE, I. R. - Vocal fold physiology San Diego, Singular, 1993.
6. HARRISON, G. A.; TROUGHEAR, R. H.; DAVIS, P.J.; WINKWORTH, A.L. - Inspiratory speech as a management option for spastic dysphonia. Ann. Otol. Rbinol. Laryngol., 101: 375-382, 1992.
7. LEHMANN, K. H.; Reverse phonation: A new maneuver of examining the larynx. Radiology, 84: 215 -21, 1965.
8. SATALOFF, R.T. - Professional voice: the science and art of clinical care. 2aed. Singular, San Diego, 1997.
9. SATO, K. & HIRANO M. - Age-related changes of elastics fibers in the superficial layer of the lamina propria of vocal folds. Ann. Otol. Rbinol. Laryngol., 106: 44-8, 1997.
10. TIMCKE R.; LEDEN, H.; MOORE, P. - Laryngeal vibrations: measurements of the glottic wave. Arch. Otololaryngol., 68., 119, 1958.ANNEX I - Protocol used for laryngeal exam to investigate Inspiratory Phonation in Characterizing Benign Laryngeal Lesion.
* Speech Pathologist and Voice Specialist, Centro de Estudos da Voz - CEV.
** Speech Pathologist and Voice Specialist, Ph.D. in Disorders of Human Communication at Universidade Federal de São Paulo, Director of Centro de Estudos da Voz - CEV.
*** Otorhinolaryngologist, Ph.D. in Otorhinolaryngology and Head and Neck Surgery at Universidade Federal de São Paulo. Head of the Sector of Head and Neck Surgery of the Service of Otorhinolaryngology at Hospital do Servidor Público do Estado de São Paulo, Francisco Morato de Oliveira.
**** Speech Pathologist and Voice Specialist, Centro de Estudos da Voz - CEV.
Preliminary version presented at The Voice Foundation Congress 27th. Annual Symposium: Care of the Professional Voice - Philadelphia - 1998. Integral version presented and awarded best Free Paper at I Congresso Triológico de Otorrinolaringologia and 5° Congresso Brasileiro de Laringologia a Voz.
Address for correspondence: Rua dos Estados Unidos da Venezuela, 78 - Santos/ SP.
Tel: (55 13) 261-3434 and 222-1543 Fax: (55 13) 219-8725.
E-mail: valente@iron.com.br
Article submitted on July 21, 2000. Article accepted on August 22, 2000.








Print: ![]()