

Year: 2000 Vol. 66 Ed. 4 - (14º)
Relato de Casos
Pages: 409 to 412
Pleomorphic Adenoma of the Nasal Septum: a case Report and a Review of the Literature.
Author(s):
José A. P. Felix*,
Sebastião Tonon*,
José C. Saddy**,
Roberto C. Meirelles***,
Felippe Felix****.
Keywords: mixed tumor, pleomorphic adenoma, nasal cavity
Abstract:
The authors describe a case of pleomorphic adenoma of the nasal septum in a 23-year-old mate patient with a round lesion, red-coloured, fixed in the anterior septal mucosa, area of Little, obstructing the right nasal cavity. The procedure used was the complete surgical removal without residual or recurrent lesion. This tumour has its origin in the salivary glands being extremely rare in the mucosa of the nasal cavity.
![]()
INTRODUCTION
Nasal tumors are infrequent. The most commonly seen in the nasal cavity are epithelial papilloma, angioma, transitional cell carcinoma, pavement carcinoma and adenocarcinoma.
Other less frequent tumors seen in the nasal fossa are divided into two categories: neural in origin (glioma, meningioma, olfactory neuroblastoma and neurilemona) and nonneural in origin (osteochondroma, chondrosarcoma, leiomyosarcoma, cystic hemangiopericytoma, adenoid carcinoma, oncocytoma and pleomorphic adenoma)12.
Pleomorphic adenoma or mixed tumor of the nasal septum was described for the first time in 1929 by Denker and Kahler13,14. Next, by Stevenson11, in 1932, and Weidlen5, in 1936. Compagno and Wong, by means of a study of the files of the institute of Pathology of American Armed Forces conducted a study of 40 cases of pleomorphic adenoma of the nasal cavity in the period between 1949 to 19743,4. It is the most commonly benign glandular tumor originated in the head and neck. It grows, in decreasing order, in the parotid gland, submandibular gland and palate7. Distant metastases and tendency to malignization are extremely rare8,9,10. Approximately 6.5% of pleomorphic adenoma occur in the minor salivary glands and are more frequent in the palate26,7. For anatomical pathological diagnosis of mixed tumor it is necessary to have two types of cells: on one side, epithelial and myoepithelial cells and on the other, stroma of fibroid, mixoid, chrondroid, vascular or mixochondroid characteristics. Treatment is surgical, either conservative or radical, depending on the progression characteristics of the tumor.
CASE REPORT
LCP, male aged 23 years old, white, born in Niteroi, RJ, came for medical assistance in 04/09/98 after having noticed red formation in the right nasal fossa. He complained about marked nasal obstruction that had made him use topic decongestant for a long time. He did not report pain, bleeding orfacial deformity. At anterior rhinoscopy we observed an oval, smooth, encapsulated and elastic tumor, non-painful and non-ulcerated, of intense pink color and mucosa highly vascularized. It obstructed the anterior part of right nasal fossa, compressing the head of right inferior concha (Figure 1). At high resolution CT scan, axial section, the tumor was well delimited on the cartilaginous region of nasal septum, without invasive process (Figure 2). On 14/01/ 99, the patient was submitted to surgical exeresis of the lesion under general anesthesia. After incision of the mucosa, we proceeded to detachment of sub-perichondrium, and noticed tumor implantation partially adhered to quadrangular cartilage. We conducted an ample resection of the lesion (Figure 3), preserving the septal cartilage, followed by 24-hour anterior packing with gauze soaked in antibiotic ointment. Post-operatively, we conducted successive dressings for crust removal. The intervention did not produce bleeding and immediate and late post-operative periods were complication-free. Histopathological analysis revealed a mucosa involving serous-mucous glands and neoplasia of small cubic cells; immersed in loose structure with extensive chondroid area (Figure 4). As a conclusion, a mixed tumor was diagnosed (pleomorphic adenoma). Six months after surgery, the patient was asymptomatic. There was total epithelization of the exposed cartilaginous area. We recommended follow-up every six months.
Figure 1. Nasal septum tumor, observed at anterior rhinoscopy.
Figure 2. At axial section, presence of tumor in the right nasal fossa.
Figure 3. Microscopic aspect of neoplasia showing glandular-type structures limited by double-layered cubic cells, amongst chondroid stroma (HE - 17.058).
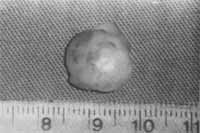
Figure 4. Surgical piece of septal tumor.
DISCUSSION
Salivary gland tumors correspond to approximately 3% of all neoplasias. Out of these, most of them are benign and about 70% are pleomorphic adenomas. Approximately 8% of pleomorphic adenomas are located in minor salivary glands and the most frequent location is the oral cavity2. According to Spirro et al. (1973),11.8% of minor salivary gland tumors are benign and only 1% of the tumors is found in the nasal cavity and nasopharynx1. There is no prevalence of sex or race10, and it may be present in any age, despite the fact that it is more frequent between the 2nd and 3rd decades of life. The most frequent location of pleomorphic adenoma in the nasal cavity is the quadrangular cartilage, followed by nasal external wall, especially in the turbinate.
As to the origin of pleomorphic adenoma of nasal septum, there are many theories about it. One says that it would have originated from embryological debris of vomer-nasal organ or Jacobson's organ, a 6mm long meatus with epithelial recovering, located in the cartilaginous portion of the septum, close to nasal-palatine orifice, which normally disappears early, but may persist in some adults (Stevenson, 1932). Other says that it would have originated from aberrant cells of recovering epithelium of nasal septum (Ersner and Saltzaman, 1944)7. A third says that it would have originated from ectopic glandular salivary tissue (Evans and Cruicksbank, 1970).
Recurrence of pleomorphic adenoma is higher in tumors in which histological analysis reveals more inixoid content, which is rare in pathologies located nasally (differently from the main glandular neoplasias)12.
Differential diagnosis should be done distinctively: in children, with dermoid cyst, encephaloceles and nasal glioma; in teenagers, with juvenile angiofibroma; and in adults, with destructive tumors such as inverted papilloma, plasmocytoma, oncocytoma, fibrous histiocytoma, esthesioneuroblastoma, neuroendocrine tumors, among others6.
As to malignant forms of mixed tumor of nasal septum, the most common is former pleomorphic adenoma carcinoma, in which epithelial components turn malignant and are capable of metastasizing6,7. Another malignant type is benign metastasizing pleomorphic adenoma, which is rare in recurrent tumors, and despite its benign histological aspect, it produces metastases that look histologically benignb. In minor salivary glands, only two cases are described: Wermuth, in the oral cavity, and Freeman, on the nasal septum7.
FINAL COMMENTS
The rare location of the lesion and the success of surgical treatment motivated the publication of this case report. Normally, minor salivary glands are located intra-orally, and they are very rare in the nasal mucosa, where they may be a result of embryological vestiges of salivary tissue.
REFERENCES
1. ATAMAN, M.; SENNAROGLU, L.; GEDIKOGLU, G.; AYAS, K. - Pleomorphic Adenoma of the Nasal Septum. Rhinology, 32: 211-2, 1994.
2. BERGSTRÖM, B.; BIORKLUND, A. - Pleomorphic Adenoma of the Nasal Septum - Report of two cases. J. Laryngol Otol., 95: 179-81, 1991.
3. COMPAGNO, J.; WONG, R. T. - Intranasal Mixed Tumors (Pleomorphic Adenomas): a Clinicopathologic Study of 40 cases. Am J Clin Pathol, 68: 213-218, 1977.
4. COULOIGNER, V.; JULIEN, N.; MOLAS, G.; STERKLERS, O. Pleomorphic Adenoma of the Nasal Septum- apropos of a case. Ann. Otolaryngol. Chir. Cervicofac., 110: 230-3, 1993.
5. ERSNER, M. S.; SALTZMAN, M. - A Mixed Tumor of the Nasal Septum - Report of a Case. Laryngoscope, 54: 287-96, 1994.
6. FRAILE-RODRIGO, J. J.; MARTINEZ-BERGANZA, Y.; ASENSIO, R.; YUS-GOTUR, C.; GARCIA-ORTIN, M.; GARCIA-ORTIN, J. Adenoma Pleomorfo de Tabique Nasal-Revision. Acta Otorrinolaringol. Esp., 44(3): 239-41, 1993.
7. FREEMAN, S. B.; KENNEDY, K. S.; PARKER, G. S.; TATUM, A. S. - Metastasizing Pleomorphic Adenoma of the Nasal Septum. Arch. Otolaryngol Head Neck Surg.. 116: 1331-3. 1990.
8. GOLZ, A.; BEM-ARIE, Y.; FRADIS, M. -Pleomorphic Nasoseptal Adenoma. J. Otolaryngol, 26(6): 399-401, 1997.
9. MAJED, M. A. - Pleomorphic Adenoma of Nasal Septum. J. O. Laryngol. Otol., 85:975-6, 1990.
10. Prager, D. A; Weiss, M. H.; Buchalter, W. L.; et al. - Pleomorphic Adenoma of the Nasal Cavity. Ann. Otol. Rhinol. Laryngol., 100:600, 1991.
11. STEVENSON, H. N. - Mixed Tumor of the Nasal Septum. Ann. Otol. Rhinol. Laryngol., 41: 563-570, 1932.
12. VALDEZATE, L. A. V.; ARGUELLES, M. E. M. - Adenoma Pleomorfo (Tumor Mixto) en el Septum Nasal. An Otorrinolaringol. Ibero Am., 21(3): 265-73, 1994.
13. WALLACE, R. D. & COLS - Pleomorphic Adenoma of the Nose. Clinical and Pathologic Head Neck Surg., 116(4):4868, 1990.
14. WORTHINGTON, P. - Pleomorphic Adenoma of the Nasal Septum. Br. J. Oral. Surg., 14: 245-52, 1977.
* Joint Professor of the Discipline of Otorhinolaryngology at Faculdade de Medicina da Universidade Federal Fluminense.
** Faculty Professor of the Discipline of Pathology at Faculdade de Medicina da Universidade Federal Fluminense.
*** Joint Professor and Coordinator of the Discipline of Otorhinolaryngology at Hospital Universitário Pedro Ernesto, Universidade do Estado do Rio de Janeiro.
**** Medical undergraduate at Universidade Federal Fluminense.
Study conducted in a private office.
Address for correspondence: Jose Antonio de Paula Felix - Rua Coronel Moreira César, 229 - Sala 1815 - Icaraí - 24230-053 Niterói /RJ - Tel / Fax: (55 21) 710-6220
E-mail: felfelix@nitnet.com.br
Article submitted on September 24, 1999. Article accepted on May 14, 2000.



Print: ![]()