

Year: 2000 Vol. 66 Ed. 4 - (12º)
Relato de Casos
Pages: 397 to 401
Empty Sella Turcique and Hyposmia: Report of a Case.
Author(s):
Nadejda M. A. V. M. Silva*,
Ney de Castro Júnior**,
Elizabeth C. M. de Araújo***,
Flávio P. de Carvalho****.
Keywords: empty sella syndrome, smell
Abstract:
The empty sella turcique is one development abnormality of sella turcique diaphragm, allowing the free communication between the spinal fluid of arachnoid space and the sella. It is frequently found in middle-aged women whose most common sympton is headache. Its diagnosis is based on radiological study which will make the difference between empty sella turcique and pituitary gland tumour, specially adenoma. The present work describes one case of Primary Empty Sella Turcique associated with Hyposmia and its bibliographic revision.
![]()
INTRODUCTION
The expression empty sella was proposed for the first time by Busch in 1951, to refer to a case in which the sella turcica examined during autopsy seemed to be empty of its hypophysial content. In 1968, Lee and Adams. designated by the expression empty sella syndrome an anatomical-radiological entity without clinical expression that varied a lot. Weiss and Raskind compared the so-called primary empty sella syndrome to empty sella turcica secondary to radiotherapy, surgical or mixed treatment of hypophysis6.
CASE REPORT
We describe the case of a female patient, white, aged 57, complaining of hyposmia for 30 days. She reported also intermittent mild and chronic headache. She did not refer any other underlying pathologies, as well as smoking or alcohol abuse.
Physical ENT exam - otoscopy, oropharyngoscopyand anterior rhinoscopy were within normal ranges.
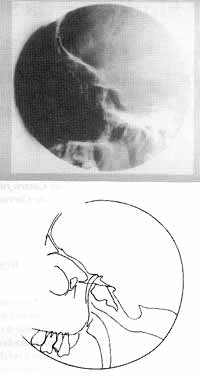
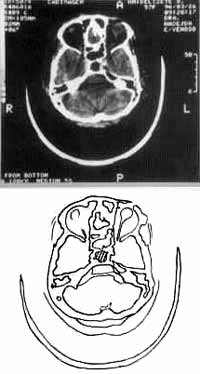
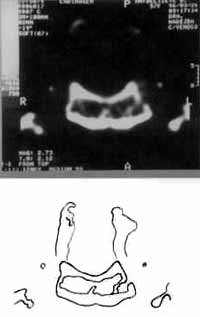
We ordered paranasal sinuses x-rays that showed enlargement of sella turcica and no sinusal abnormality (Figure 1). We then ordered head CT scan in order to exclude the hypothesis of expansive process at pituitary gland. CT scan confirmed the enlargement of sella turcica and the presence of liquid inside it, contributing to the final diagnosis of primary empty sella syndrome (Figures 2, 3, 4 and 5).
LITERATURE REVIEW
Hypophysis gland is a complex structure that lies in a walled bone cavity, the sella turcica, on the sphenoid bone on the skull base2.
Sella turcica is separated anteriorly from the cranial cavity through a resistant reflection of dura, the sella diaphragm, and through it the hypophysis stem and blood vessels reach the main structure of the gland2.
Due to its situation, information regarding volume and structure of hypophysis may be obtained during life only through x-rays2. The sella turcica is normally 12mm deep and 15mm long on the lateral projection of x-rays5. Its normal regular shape is round or ovoid, and less frequently, it is shallow and flat5. Owing to the difficulty of measuring precisely because of indistinct bone margins, radiological dimensions of sella turcica are described with semi-quantitative estimates as enlarged, normal or borderlines.
As to regular radiological methods, we noticed that at conic inferior incidence it is possible to see the first indication of empty sella syndromes; CT scan, on the other hand, allows excellent visualization of hypophysial parenchyma, shows the supra-sellar extension and enables detection of empty sella, which does not require in most of the cases intra-thecal contrast with metrizamide2, 5.
Figure 1. Rx and drawing of paranasal sinuses, profile incidence, with enlargement of sella turcica.
Primary empty sella syndrome is a development anomaly of the diaphragm of sella turcica, allowing for free communication of arachnoid CSF with the sella2,5,6. In its most extreme level, there is only a small layer of hypophysial parenchyma on the floor of the fossa2 (Figures 6 and 7).
Despite the reduction of hypophysial mass, clinical and lab evidence of hypopituitarism is uncommon2,5, and it is frequently found in middle-aged hypertensive women who are slightly obese and complain of headache5 (caused by the pressure over the adjacent structures such as sellar diaphragm, dura and walls of large vessels). The diagnosis is performed radiologically, manifested as a symmetric ballooning of the sella with minimal backward deviation of posterior clinoid at lateral skull incidence2.
Differential diagnosis of an enlarged sella turcica in cludes hypophysial tumor, craniopharyngeoma, target-organ failure with hypophysial hyperplasia (diabetes insipidus, hypopituitarism and adrenal failure), empty sella syndrome and lesions that deviate sellar architecture, such as meningeoma, chordoma, distant metastasis and others5.
Figure 2. CT scan and drawing at coronal section, confirming the enlargement of sella turcica (highlighted in the drawing).
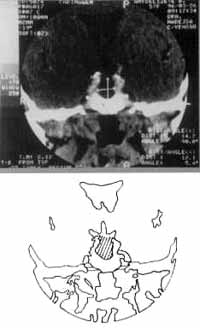
Figure 3. CT scan and drawing showing the increased measures of sella turcica.
If the diagnosis of sellar enlargement is confirmed radiologically, the absence of endocrine abnormalities in lab and clinical exams increases the likelihood of having primary empty sella syndrome2,5, despite the fact that any configuration may be found in hypophysial tumors and empty sella5. Until recently, the differentiation between empty sella and hypophysial adenomas required displacement of sellar liquid with air (pneumoencephalography) with or without metrizamide. The headache and discomfort caused by this procedure may be avoided by using high-resolution CT scan, which distinguishes between a sella full of liquid and a sella that houses an adenoma2.
If there is hypothesis of hypophysial tumor, basal endocrine assessment depends on sericT4, TSH, testosterone or stradiol, LH, FSH, 17 24-hour urine hydroxisteroids and seric prolactin. High seric levels of prolactin, associated with enlargement of sella, strongly suggest the presence of hypophysial tumor; however, minimal elevations of prolactin seric concentrations are occasionally seen in cases of empty sella5.
Compromise of 3rd, 4th and 6th cranial nerves is present in 10 to 20% of the patients with macroadenoma, but affection of the 3rd cranial nerve is more frequently seen 2. Sometimes, olfactory nerves are also affected by tumor growth or transfrontal hypophysial surgery resulting in loss of smell2, what motivated us to study the present case (Figure 8).
FINAL COMMENTS
Since it is a frequent complaint present in the symptomatology of various etiologies, hyposmia should always be correctly investigated.
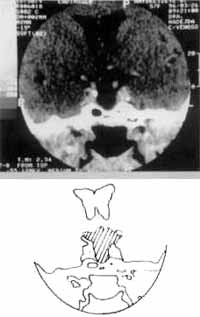
Figure 4. CT scan with contrast and drawing, without pathological reinforcement of tumor.
Figure 5. CT scan section showing liquid content occupying sella turcica (x-ray and drawing).
Figure 6. Normal representation of the relation between meninges and hypophysis. 1) - dura, 2) - pia, 3) - arachnoid mater.
Figure 7. Herniation of arachnoid through sellar incompetence (empty sella).
Representative drawings of Figures 6 and 7 were reproduced from JORDAN, R.M.; KENDALL, J.W.; KERBER, C. W. - The primary empty sella syndrome: Analysis of the clinical characteristics, radiographic features, pituitary function, and cerebrospinal fluid adenohypophysial hormone concentrations. Am. J. Med., 62: 569, 1977.
(FIGURA 8, PÁG. 401)
Figure 8. Transversal section of the skull showing the atomical relation of sella turcica, optic chiasm and olfactory tract.
We noticed that the association between hyposmia and primary empty sella syndrome is rare and we could not correlate them as cause and effect, as confirmed by the literature in the past 30 years.
We would like to highlight the importance of correlating different medical specialties, as required in the case reported here.
REFERENCES
1. ARON, D. C. FINDLING, J. W.; TYRRELL, J. B. - Hypothalamus & Pituitary. In: GREENSPAN, F. S.; STREWLER, G. J. - Basic & Clinical Endocrinology, Stamford, Appleton & Lange, 5. Edition, 1997, 123 - 24.
2. DAUGHADAY, W. H. - A Hipofise Anterior. In: WILSON, J. D.; FOSTER, D. W. - Williams, Tratado de Endocrinologia, Dallas, Manole Ltda, 1988, 704 - 34.
3. HEIDEGGER, G. W. - Atlas de Anatomia Humana, 3a Edição, Basel, Guanabara Koogan, 1971, 72 - 3.
4.. JORDAN, R. M.; KENDALL, J. W.; KERBER, C. W. - The primary empty sella syndrome: Analysis of the clinical characteristics, radiographic features, pituitary function, and cerebrospinal fluid adenohypophysial hormone concentrations. Am. J. Med., 62: 569, 1977.
5. MALARKEY, W. B. - A Hipofise a o Hipotalamo. In: MAZZAFERRI, E. L. - Endocrinologia, Nevada, Guanabara Koogan, 1982, 16 - 35.
5. PETRUS, M.; BONAFE, A.; DUTAU, G.; MANALFE, C.; ROCHICCIOLI, P. - Syndrome de la selle turcique vide primitive. Etude de deux cas. Arch. Fr. Pediatr., 38 (8): 581- 6, 1981.
* Faculty Professor of the Discipline of Otorhinolaryngology at Escola de Ciências Médicas de Volta Redonda, Master Degree under way with Post-Graduate Course in Otorhinolaryngology at Santa Casa de São Paulo.
** Professor, Head of the Clinic at the Department of Otorhinolaryngology, Santa Casa de São Paulo.
*** Assistant Professor of the Discipline of Otorhinolaryngology at Escola de Ciências Médicas de Volta Redonda.
**** Odonthologist (Responsible for the figures displayed in the case study).
Study conducted at Escola de Ciências Médicas de Volta Redonda/ RJ.
Address for correspondence: Dra. Nadejda Maria Ávila Varginha de Moraes a Silva - Escola de Ciências Médicas de Volta Redonda - Fundação Oswaldo Aranha. Estrada Volta Redonda/Pinheiral, 1325 - Três Poços - 27251-970 Volta Redonda/ RJ - Tel/ Fax: (55 24) 346-8400 and 346-8223.
Article submitted on July 19, 1999. Article accented on September 23, 1999.
Print: ![]()