

Year: 2000 Vol. 66 Ed. 4 - (2º)
Artigos Originais
Pages: 317 to 324
Audiological Evaluation in Children Born to HIV Positive Mothers.
Author(s):
Carla G. Matas*,
Ana P. Sansone**,
Maria C. M. Iorio***,
Regina C. M. Succi****.
Keywords: hearing, hearing tests, children, acquired imunodeficiency syndrome, otitis, central hearing loss
Abstract:
Purpose: The aim of the present study was the audiological evaluation of children born to mothers serologically positive for HIV, in order to verify the occurrence of auditory disorders. Material and method: The population studied included 143 children - 82 males and 61 females - ranging in age from one month to two years and six months. The children were divided into three groups, following the revised classification systemt1 for human immunodeficiency virus infection in children less than 13 years of age, as infected (1), seroreverter (SR) or exposed (E). The audiological evaluation procedures employed were behavioral observation audiometry, visual reinforcement audiometry and acoustic immittance measurements. Analysis of the sample population for duration of gestation and birth weight showed that the majority of the children were born at term with a suitable weight for gestational age. For studying the incidence of auditory disorders, the results of the latest audiological examinations on the 143 children were used. Results: Statistical analysis showed a significantly higher incidence of auditory disorder in the infected children. Among the seroreverter and exposed children the inverse was the case, with the majority of the children showing no auditory disorder. Conclusion: Results suggesting central auditory disorders were predominant in the infected group, whereas the incidences of central and middle ear disorders were similar in the other two groups.
![]()
INTRODUCTION
Acquired immunodeficiency syndrome - AIDS is caused by human immunodeficiency virus - HIV, described for the first time in 1983 as the etiological agent responsible for the severe impairment of immune response in subjects with AIDS8.
The first cases of AIDS were described by Centers for Disease Control and Prevention (CDC) in 1981, in Los Angeles and New York.
As the disease evolves, the subject will develop severer immunological deficiencies and will be affected by innumerous opportunist infections.
HIV routes of transmission are clearly stated: blood transfusion, occupational accident, use of injecting drugs, sexual intercourse and perinatal trasmission12.
Most of the cases of HIV in children were transmitted perinatally28,21, because the virus is transmitted from the infected mother into the fetus or the newborn.
Perinatal transmission may take place during gestation (in the uterus), during delivery (intra-delivery), or post-delivery12,21. The specific rate of transmission of HIV during gestation, delivery or post-delivery has not been established yet28,21, although recent data have suggested that it is more important at the end of gestation and in the intra-delivery period.
Diagnosis of HIV infection in newborns born to HIV-infected mothers is difficult because of the presence of maternal anti-HIV IgG antibodies, which cross the placenta barrier and reaches fetal circulation22. At birth, most of these children have positive antibody to HIV and only 15 to 30% of them will be in fact infected. Maternal antibody normally becomes undetectable at about 9 months of age, but it still may be detected up to 18 months of age.
Diagnosis of HIV infections in newborns of HIV-infected mothers is only confirmed by 2 positive results in tests of viral detection or viral antigen, from two distinct blood samples. On the other hand, for a child to be considered non-infected, he or she should present negative results in two distinct blood samples of tests or be followed up until all maternal antibodies disappear23.
The first suggestive case of AIDS in children was described by CDC in 1982. In 1983 the first reports of AIDS in children infected perinatally were published20,25. From then on, various studies have been conducted in order to determine the clinical evolution of HIV infection in the pediatric population, because in children the infection seems to be more aggressive, with shorter periods of latency between infection and onset of symptoms, in addition to shorter period of survival after the surge of symptoms, if compared to adult population26.
Among the innumerous infections that may affect HIV-infected children, we can point out upper airway infections, especially sinusitis and middle and external otitis26,16,13,17.
We know that external and middle otitis may cause temporary peripheral hearing loss and it should be identified as early as possible in order to have effective medical treatment.
It is known as well that as the disease progresses, there is a progressive impairment of central nervous system, including central auditory system because of the direct action of the virus over the structures of central nervous system, affecting the maturational process or resulting from opportunist infections16,17,5.
Therefore, we expect to find abnormal results in tests that assess central auditory processing, reflecting difficulties of attention, discrimination, recognition and comprehension of auditory information6.
In addition to abnormal results in central auditory tests, there are also electrophysiological alterations in evoked potentials of the brainstem-ABR and cognitive auditory potential (P 300)5,6.
Taking into account the importance of the integrity of peripheral and central auditory systems for acquisition and development of speech, language and learning, it is essential to early identify and treat both peripheral and central auditory disorders in the pediatric population in order to improve quality of life and provide basic conditions for these children to communicate effectively in their environment.
Knowing that children born to HIV-infected mothers are more likely to have otitis or to be poorly-stimulated because of health status of mothers, the present study aimed at assessing children born to HIV-positive mothers, checking the occurrence of hearing disorders.
MATERIAL AND METHOD
This study was conducted at the Ambulatory of the Discipline of Human Communication Disorders of the Department of Otorhinolaryngology and Human Communication Disorders at Escola Paulista de Medicina, Universidade Federal de São Paulo.
The population under study consisted of 143 children, 82 male and 61 female patients, ages ranging from one month to 2 years and 6 months.
All studied children were born to HIV-infected mothers and were being followed-up at the Discipline of Pediatric Infectology of the Department of Pediatrics at Escola Paulista de Medicina; Universidade Federal de São Paulo.
Children were divided into 3 groups according to the Revised Classification System 199410, for infection with HIV in children below 13 years of age.
The first group, called perinatally exposed (E), consisted of 34 children aged younger than 18 months born to HIV-infected mothers who had positive results to anti-HIV antibodies.TABLE 1 - Levels of reference used to interpret the results of reflex and innate automatism and stages of auditory processing in children aged zero to 24 months of age18.
RCP = cochleo-palpebral reflex
The second group, called serum-reverted (SR), was formed by 91 children aged older than 6 months who had two or more negative results for anti-HIV antibodies.
The third group, called HIV-infected (I), was formed by 18 children of up to 2 years and 6 months who definitely had HIV infection (presence of positive anti-HIV antibodies after 18 years and/or viral detection and/or clinical manifestations that defined AIDS).
In our study of auditory disorders in children born to HIV-infected mothers we used the results of the last hearing assessment conducted in each of the 143 studied children.
Based on data collected for anamnesis and otoscopy carried out by the pediatrician, we started auditory assessment using different procedures according to age range and clinical status of the child. The procedures used were:
1) Behavioral audiometry
2) Audiometry with visual reinforcement
3) Acoustic immitance audiometry
1) Behavioral audiometry
The observation of behavioral responses to different instrumental stimuli was carried out in children aged between 1 and 24 months1.
Instrumental sound stimuli used were rattle I, rattle II, Brazilian notched bamboo instrument (reco-reco), bell, cylinder shaped rattle (ganza), small attached cymbals, cymbals, Brazilian doubled bell instrument (agogo), and drums.
The responses obtained were classified as follows1:
1. Reflex responses and-innate automatism - cochleopalpebral reflex, Startle reflex.
2. Stages of auditory processing - attention to sound, look for sound source, lateral localization, localization of sounds downward and upward (direct and indirect).
The levels of reference used to interpret the results of behavioral auditory assessment are presented in Table 1.
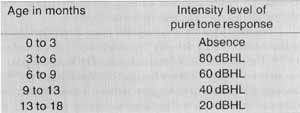
Response patterns suggestive of central auditory disorders were: exacerbated response, increase latency of response, difficulty to locate sound despite normal hearing, absence of adaptation to repetitive stimuli, absence of cochleo-palpebral reflex in the presence of normal hearing4.TABLE 2 - Levels of reference used to interpret the results of minimum level of response for pure tone in children aged zero to 24 months of age18.
dBHL = hearing level decibel
2) Audiometry with visual reinforcement.
The investigation of minimal thresholds for modulated pure tones was conducted in children aged from 3 to 24 months of age, using Pediatric audiometer model PA2, Interacoustics1.
Levels of reference are presented in Table 2.
3) Acoustic immitance audiometry
Acoustic immitance audiometry was carried out with Handtymp equipment, Damplex, and tympanometric curve and ipsilateral stapedial reflex were investigated at 95 dB SPL in frequencies 500, 1.000, 2.000 a 4.000 Hz bilaterally.
In order to interpret the results of tympanometric curve, we used the classification proposed by Jerger (1970)14.
As to acoustic reflex of stapedial muscle, they were considered absent or present at the intensities investigated by the equipment.
The results obtained in the audiological assessment allowed us to make diagnostic hypotheses about hearing disorders, described in Table 3.TABLE 3 - Interpretation of results of audiological assessment18
RESULTS AND COMMENTS
We initially characterized the studied population as to duration of gestation and weight at birth (Tables 4 and 5). Most of the children assessed were delivery in term and had adequate weight for gestational age.
Studies of occurrence of hearing disorders in infected children (I), serum-reverted (SR) and exposed to HIV (I).
The results obtained in the last hearing assessment of 143 children subdivided into 3 groups previously defined are presented in Table 6.
There was statistically significant predominance of hearing disorders in the infected group and in the remaining groups (serum-reverted and exposed) the opposite happened, that is, predominance of absence of hearing disorders.
Other studies conducted with children also showed higher occurrence of hearing disorders in groups of HIV-infected children16,17,27.
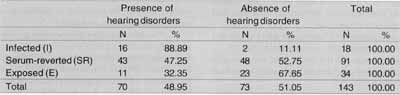
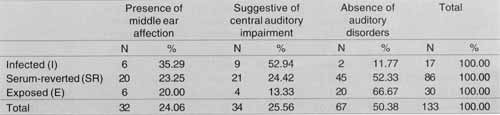
Next, we presented the results of hearing assessment specifying type of hearing disorder (Table 7).
In the infected group we found predominance of alterations suggestive of central auditory disorder and in serum-reverted and exposed groups there was similarities between middle ear affections and suggestive central auditory disorders.
Some studies from the literature mentioned higher incidence of middle ear affections in HIV-infected children 16,7 a fact present also when taking into account the incidence of middle ear alterations in HIV serum-reverted and exposed children16,7.
In other studies, it was noticed that HIV infections do not seem to increase the incidence of middle ear affections, but rather predispose to its recurrence15,24.
The data we collected concerning predominance of suggestive central auditory disorder in HIV-infected children were compatible with data obtained by Belman et al. (1985)9, Musolino (1996)18 and Succi et al. (1996)27. In some cases, the procedure used for detection of central auditory disorders was brainstem auditory evoked potentials8,18, whereas only one study used the same procedure used here, that is, behavioral audiometry27.
Next, we performed analysis of data dividing the sample as to duration of gestation (pre-term and in term children) and weight at birth (adequate for gestational age or small for gestational age).
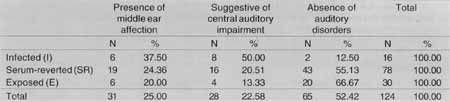
In term delivery babies we, found statistically significant predominance of hearing disorders in the infected group, whereas in serum-reverted and exposed groups absence of hearing disorder was predominant. The most frequent hearing disorders in the affected group were suggestive of central auditory disorders, and in serum-reverted and exposed groups, both middle ear affections and suggestion of central auditory disorder results were similar (Table 8).TABLE 4 - Distribution of samples as to duration of gestation, in the 3 groups of children assessed: infected fl). serum-reverted (SR) and exposed (E).
TABLE 5 - Distribution of sample according to weight at birth in the 3 groups of children assessed: infected (I), serum-reverted (SR) and exposed (E).
AIG - adequate for gestational age
PIG - small for gestational age
GIG - big for gestational age
TABLE 6 - Study of occurrence of hearing disorders in children born to HIV-positive mothers according to status of HIV infection.
Qui-square test
X2 calculated = 15.343*
X2 critical = 5.991
Partition of Qui-square
SR+E Vs I X2 calculated = 13.144*
E Vs SR X2 calculated = 2.199 INS.
X2 critical = 3.84
For pre-term babies, we observed that absence of hearing disorders was more marked only for the exposed group. The type of hearing disorder most frequently found both for infected and exposed groups was suggestive of central auditory processing disorder (Table 9).
Comparing term born babies to pre-term babies, we observed difference in the behavior of serum-reverted groups: the presence of more hearing disorders in pre-term serum-reverted children, usually central in nature. This finding is in agreement with data by Azevedo (1993)3 who studied hearing development of term and pre-term babies and observed significant difference in the hearing development of these two groups, because pre-term babies had delay in the stages of hearing development, a piece of data that suggested central auditory processing disorder.
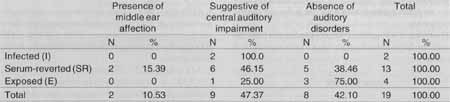
For children with suitable weight for gestational age, similarly to what happened with term babies, we observed statistically significant predominance of central hearing disorders in the infected group. In serum-reverted and exposed groups there was similarity between the results of middle ear affections and suggestion of central auditory disorders (Table 10).TABLE 7 - Distribution of the occurrence of middle ear affection and suggestive alterations of central auditory processing in children born to HIV-positive mothers according to status of HIV infection.
TABLE 8 - Distribution of the occurrence of middle ear affection and suggestive alterations of central auditory processing in children born to HIV-positive mothers at term delivery.
TABLE 9 - Distribution of the occurrence of middle ear affection and suggestive alterations of central auditory processing in children from pre-term delivery born to HIV-positive mothers.
In low birth children for gestational age, we noticed absence of hearing disorders in serum-reverted and exposed groups, with predominance of disorders suggestive of central auditory impairment in the infected group (Table 11).
In summary, based on the results obtained in the present study we detected differences between development of auditory behavior in infected and serum-reverted children or exposed children born to HIV-infected mothers.
Northern and Downs (1984)19 describing congenital infections under the acronym of TORCH (toxoplasmosis, rubella, cytomegalovirus, simple herpes) reported that they may cause auditory impairment, which can be either central or peripheral and progressive or non-progressive.TABLE 10 - Distribution of the occurrence of middle ear affection and suggestive alterations of central auditory processing in children delivered with weight adequate for gestational age born to HIV-positive mothers.
TABLE 11 - Distribution of the occurrence of middle ear affection and suggestive alterations of central auditory processing in children delivery with low weight to gestational age born to HIV-positive mothers.
We observed that, similarly to other congenital infections, HIV infection seems to be a high risk factor for central auditory disorders.
Therefore, it is suggested that congenital infection by HIV should also be included as a risk factor for development of hearing disorder.
CONCLUSION
Based on the critical analysis of data obtained in the present study we concluded that: infected children had predominance of hearing disorders, most of them suggestive of central impairment, whereas in serum-reverted and exposed children there was predominance of absence of auditory disorders.
REFERENCES
1. AZEVEDO, M. F. - Avaliação subjetiva da audição no primeiro ano de vida Temas sobre Desenvolvimento, 1 (3):11-4, 1991.
2. AZEVEDO, M. F. -Avaliação audiológica no primeiro ano de vida. In: Lopes Fo., O. - Tratado de Fonoaudiologia.1ª. edição. São Paulo, Roca, 1997. p.239-63.
3. AZEVEDO, M. F. - Desenvolvimento auditivo de crianças normais a de alto risco: estudo comparativo das respostas comportamentais a estímulos sonoros. São Paulo, 1993. (Tese - Doutorado-Universidade Federal de São Paulo - Escola Paulista de Medicina)
4. AZEVEDO, M. F.; PEREIRA, L. D.; VILANOVA, L. C. P.; GOULART, A. L. -Avaliação do processamento auditivo central: identificação de crianças de risco para alteração de linguagem e aprendizado durante o primeiro ano de vida. In: Marchesan, I.Q.; Bolaffi, C.; Gomes, I. C. D.; Zorzi, J.L. (eds.)- Tópicos em Fonoaudiologia. São Paulo, Lovise, 1995. V.II: p.447-62.
5. BANKAITIS, A. E.; CHRISTENSEN, L. A.; MURPHY, G.; MOREHOUSE, C. R. -HIV/AIDS and auditory evoked potentials. Seminars in Hearing, 29(2):177-93, 1998.
6. BANKAITIS, A. E. & KEITH, R. W. - Audiological changes associated with HIV infection. Ear Nose Throat J., 74(5):3.539, 1995.
7. BARNETT. E. D.: KLEIN. J. O.: PELTON. S. L: LUGINBUHL. L. M. - Otitis media in children born to human immunodeficiency virus - infected mothers. Pediatr. Infect. Dis. J., 11(5): 360-4, 1992.
8. BARRÉ-SINOUSSI, F.; CHERMANN, J. C.; REY, F.; NUGEYRE, M. T.; CHAMARET, S.; GRUESTJ; DAUGUET, C.; AXLER-BLIN, C.; VEZINET-BRUN, F.; ROUZIOUX, C.; ROZENBAUM, W.; MONTAGNIER, L. - Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science (Wash.), 220: 868-71, 1983.
9. BELMAN, A.L.; ULTMANN, M.H.; HOROUPIAN, D.; NOVICK, B.; SPIRO, A J.; RUBINSTEIN, A.; KURTZBERG, D.; CONEWESSON, B. - Neurological complications in infants and children with acquired immune deficiency syndrome. Ann. Neurol., 18:560-6, 1985.
10. CENTERS FOR DISEASE CONTROL AND PREVENTION - 1994 Revised classification system for human immunodeficiency virus infection in children less than 13 years of age. MMWRMorb. Mortal. Wkly. Rep., 43(No. RR-12):1-9, 1994.
11. CRAVEN, D.E.; STEGER, K.A.; JAREK, C. - Human immunodeficiency virus infection in pregnancy: epidemiology and prevention of vertical transmission. Infect. Control Hosp. Epidemiol., 15(1) 36-47, 1994.
12. FRIEDLAND, G.H. & KLEIN, R.S. -Transmission of the human immunodeficiency virus. N. Engl. J Med., 317(18):1125-35, 1987.
13. GOLD, S. & TAMI, T.A. - Otolaryngological manifestations of HIV/AIDS. Seminars in Hearing, 19(2):165-75, 1998.
14. JERGERJ. -Clinical experience with impedance audiometry. Arch. Otolaryngol., 92:311-24, 1970.
15. JOHNSON, J.P.; NAIR, P.; HINES, S.E.; SEIDEN, S.W.; ALGER, L.; REVIE, D.R.; O'NEIL, K.M.; HEBEL, R. - Natural history and serologic diagnosis of infants born to human immunodeficiency virus-infected women. Am. J. Dis. Child., 143:1147-53, 1989.
16. MADRIZ, J J. & HERRERA, G. - Human immunodeficiency virus and acquired immune deficiency syndrome AIDS - related hearing disorders. J. Am; Acad. Audiol., 6(5):358-64, 1995.
17. MATKIN, N.D.; DIEFENDORF, A.O.; ERENBERG, A. - Children: HIV/AIDS and hearing loss. Seminars in Hearing, 19(2):143-53, 1998.
18. MUSOLINO, C.V. - Avaliação audiológica de crianças portadoras do vírus HIV adquirido por transmissão vertical. São Paulo, 1996. (Tese - Mestrado - Pontifícia Universidade Católica de São Paulo).
19. NORTHERN, J.L. & DOWNS, M.P., ed. -Hearing in Children. 3ª. ed. Baltimore, Williams & Wilkins, 1984. 391p.
20. OLESKEJ; MINNEFOR, A.; COOPER, R.; THOMAS, K.; DELA CRUZ, A.; AHDIEH, H.; GUERRERO, I.; JOSHI, V.V.; DESPOSITO, F. - Immune deficiency syndrome in children. JAMA, 249(17):2345-9, 1983.
21. ORLOFF, S.L.; SIMONDS, R j.; STEKETEE, R.W. & ST. LOUIS, M.E.-Determinants of perinatal HIV-1 transmission. Clin. Obstet. Gynecol., 39(2):386-95, 1996.
22. PAHWA, S. - Human immunodeficiency virus infection in children: nature of immunodeficiency, clinical spectrum and management. Pediatr. Infect. Dis. J., 7.S61-S71, 1988.
23. PECKHAM, C. & GIBB, D. -Mother-to-child transmission of the human immunodeficiency virus. N. Engl J Med., 333(5): 298-302, 1995.
24. PRINCIPI, N.; MARCHISIO, P.; TORNAGHI, R.; ONORATO, J.; MASSIRONI, E.; PICCO, P. - Acute otitis media in human immunodeficiency virus - infected children. Pediatrics, 88(3):566-71, 1991.
25. RUBINSTEIN, A.; SICKLICK, M.; GUPTA, A.; BERNSTEIN, L.; KLEIN, N.; RUBINSTEIN, E.; SPIGLAND, L; FRUCHTER, L.; LITMAN, N.; LEE, H.; HOLLANDER, M. - Acquired immunodeficiency with reversed T4/T8 ratios in infants born to promiscuous and drug-addicted mothers. JAMA, 249(17): 2350-6, 1983.
26. SCULERATI, N. & BORKOWSKY, W. - Pediatric human immunodeficiency virus infection: an otolaryngologist's perspective. J. Otolaryngol., 19(3):182-8, 1990.
27. SUCCI, R.C.M.; MATAS, C.G.; SANSONE, A.P.; IORIO, M.C.M.; MACHADO, D.M. - Auditory disorders in children born to HIV positive mothers. In: WORLD CONGRESS, 1; INTERAMERICAN OF PEDIATRIC INFECTIOUS DISEASES, 15, Acapulco, Mexico, 1996. Abstracts. Mexico, World Society of Pediatric Infectious Diseases, 1996. p.9.
28. WILLOUGHBY, A. - Epidemiology of human immunodeficiency virus infection in children. Ann. Allergy, 72:185-92. 1994.
* Joint Professor of the Course of Speech and Hearing Pathology at Faculdade de Medicina da Universidade de São Paulo.
** Master degree under course at the Discipline of de Hearing Disorders of the Department of Otorhinolaryngology / Human Communication Disorders at Universidade Federal de São Paulo - Escola Paulista de Medicina.
*** Joint Professor and Head of the Discipline of Hearing Disorders of the Department of Otorhinolaryngology / Human Communication Disorders at Universidade Federal de
São Paulo - Escola Paulista de Medicina.
**** Joint Professor of the Discipline of Pediatric Infectology of the Department of Pediatrics at Universidade Federal de São Paulo - Escola Paulista de Medicina.
Study conducted at the Discipline of Hearing Disorders of the Department of Otorhinolaryngology /Human Communication Disorders at Universidade Federal de Sao Paulo - Escola Paulista de Medicina.
Address for correspondence: Carla Gentile Matas - Avenida Damasceno Vieira, 840 - Apto. 83 - Vila Mascote - 04363-040 - Sao Paulo /SP.
Article submitted on July 28. 1999. Article accented on September 23, 1999.



Print: ![]()