

Year: 1983 Vol. 49 Ed. 2 - (3º)
Artigos Originais
Pages: 31 to 35
Author(s): R. SHIMOOKA Y HARADA 1
![]()
ABSTRACT
The epitheliail layer of the middle ear, a modified respiratory epithelium, lias an ímportant role in the defense system; under inflammatory or pathological conditions this mucosa may undergo some protective changes. Mucosal specimens of the middle ear from patients who had chronic otitis media were studied and compared with specimens of normal middle ear using SEM. The epithelia were usually thick and the surface structure varied depending upon the place the biopsy as was taken. Moreover, the structure was not uniform even un the same biopsy; areas with great proliferation of secretory cells, other areas with high population of ciliated cells and areal with loss of superficial layer were observed.
There were less ciliated cells than we expected. They were not homogeneously distributed, except for the Eustachian tube region. Most of this ciliated cells were morphologically normal, however a few isolated atrophic ones were also found.
Cholesteatoma cases showed squamous epithelia with desquamating flat keratinized cells.
MATERIAL AND METHOD
Small pieces of mucosa (2 nun x 2 mm) [from 24 patients (I case of autopsy)] were taken. Specimens were removed using a delicate biting forceps from promontory, antrum, mastoid and the Eustachian tube region.
Patients were: 13 males and 11 females (2/5-10 years; 1/10-15 years;14/25-40 years and 7/more than 40 years).
They were classifúed as follow:
1) Normal middle ear 4 (case: l, 11, 20, 22).
2) Cholesteatoma 8 (case: 3, 4, 9,10, 13, 16, 17, 21, 23). 3) Chronic otitis media with effusion 5 (case: 7, 8, 12, 14,19).
4) Chronic otitis media without effusion 5 (case: 2, 5, 6, 15,18, 24).
Normal cases were studied as control (1 case of autopsy and 3 from patients who underwent facial nerve decompressiom The other 20 cases were from patients with chronic otitis media who underwent tympanoplasty of different types or mastoidectomy.
The specimens were immediately fixed in cold (5°C) 2% glutaraldehyde for 2 hours and post fixed in cold (5°C) buffered 2% osmiun tetroxide for 1 hour. They were dehydrated in increasing concentration of ethanol, transferred to isoamyl acetate and critical point dried using liquid CO². The specimens were coated with gold and examined with the SEM JSM-T200.
RESULTS
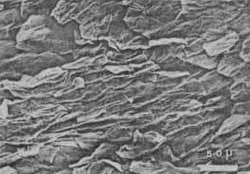
Cholesteatoma: The predominam fique was squamous epithelia with wrinkled superficial cells. Flat desquamated and keratinized cells were also found in many arcas (Fig. 1). This finding was observed not only in the cholesteatoma capsule but also in the mucous membrane of the promontory, antrum or mastoid.
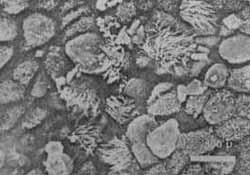
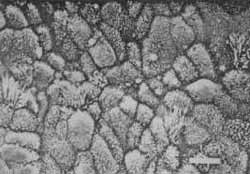
In case 9, it was found that the promontory was paved by flat polygonal cells, wíth well demarcated cell borders. They were covered by short microvilli resembling that of a mastoid mucous membrane. There were also some arcas with loss of its superficial layer which exposes underlying biconvex cells. Chronic otitis media with effusion: in antrum we found great proliferafon of non-ciliated cells. Most of them were of secretory type. There were many arcas with bulked "cauhflower" like epithelia (Fig. 2). Cells were convex and with well demarcated borders in some arcas. Most of these cells were covered with microvilli; however, there were other cells which had no microvilli at the top of their surface. Also it was possible to see these cells secreting mucus in many arcas (Fig. 3).
Fig. 1 - Cholesteatoma, squamous epithelium There are many jlat desquamated cells.
Fig. 2 - Bulked epithelium, most of cells are non-cifated with microvilli but there are a few oves without microvilli. (from antrum)
Fig. 3 - Nonciliated cells without microvilli at the top of their surface, which are secreting mucus. (from antrum)
We found isolated concentrations like "islands" of ciliated cells, surrounded by non-ciliated cells with long microvilli. They were mainly in places where surface of the epithelia presented concavities. This appearance of the epithelia resemble that of the anterior part of the tympanic cavity.
In many arcas, cells were disordered and the space between each cell seemed to be increased. Ciliated cells in these arcas did not stand upright but they looked like going to be exfoliated (Fig. 4). Cilia were disarrayed and splayed in some cases. A few ciliated cells already lacked their cita (Fig. 5).
Arcas with loss of its superficial layer exposed the polyhedral or fusiform cells. These cells were disposed in two or three layers; most of them were covered with granules of mucus (Fig. 6).
In mastoid, cells were more convex than flat. In many cases the mucous membrane resembled the antrum epithelium; there were great proliferation of secretory cells with bulked epithelium, cells wìth short microvilli and others without microvilli which secrete mucus.
There were also areas with great concentratíon of ciliated cells surrounded by non-ciliated cells with long microvilli. In the promontory, mucous membrane was not uniform in fashion, mostly populated by non-ciliated cells. Convex cells of different sizes covered with short microvilli and few isolated ciliated cells were seen.
The predominam picture was that in many areas mucous membrane lost its superficial layer exposing basal cells (fusiform shaped cells disposed in two or three layers. Sometimes basal cells resting on the basement membrane were possible to see) (Fig. 7).
Fig. 4 - Cens are disordered and look Me they are going to be exfoliated. (from antrum)
Fig. 5 - Ciliated cell which has lost most of its cilia.
Fig: 6 - Mucous membrane which has lost its superficial layer. (from promontory)
Fig. 7 - Basal cells resting on the basement membrane. (from promontory)
In the Eustachian tube region, the mucous membrane was populated mostly by ciliated cells but in lower density comparing to the mucosa in normal condition. Non-ciliated cells were seen in considerable quantity.
In the mucous membrane of the antrum of the case 8, lhe epithelium was populated by cylindrical cells, with microvilli at the top of their surface and with great space between each cell; some ciliated cells seemed that they were going to be exfoliated. Other areas were populated by convex cells without microvilli.
Chronic otitis media without effusion: in lhe promontory mucous membrane, the superficial layer in many areas was lost, thus exposing basal cells resting on lhe basement membrane. Other areas of epithelium were paved by convex cells of different size, which were covered with short microvilli. Also some areas with disorganized cell pattern were seen.
Antrum, mastoid and Eustachian tube region showed almost normal mucous membrane.
In two cases, biopsies were taken from patients who underwent second operation in which the silicon sheet was removed from the promontory. The mucous membrane appeared uniform; it was paved by convex cells with microvilli and a few ciliated cells in the first case (Fig. 8). Convex cells with long microvilli were in the second case.
Fïg. 8 - Epithellum paved by convex cells and a few cifiated cells (from promontory)
DISCUSSION
We found basically two kinds of cells in the mucous membrane surface:
1) Ciliated cells and 2) Non-ciliated cells.
The epithelia in most cases looked like a carpet with a few "holes". These holes were due to lack of superficial layer of the epithelia, so other kinds of cells such as intermediate and basal cells could be seen.
The non-ciliated cells, considered potencially secretory cells (Hentzer E., 1976), vary considerably in their size and shape; they can be cuboidal or cyhndrical. Under SEM view, it is not possible to determine if these non-ciliated cells are secretory or not, and if they have dark or light granules (according to TEM studies, Hentzer E.,1972,1976; Lim L,1976; Moller P. & Dallen H., 1981).
Almost all the surface cell of the middle ear mucosa were covered with microvilli; the microvilli were short in most cases but they were tall around islands of ciliated cells. Sometimes cells with a few microvilli (only in their boundaries) were found (as same as Friedmann L, 1981, reported).
It is known that ciliated cells proliferate under condition of secretory otitis media (Friedmanrl I. & Bird E.,1981; Shimada T. & Lim L,1972), however they also could be decreased under the same condition (Hentzer E., 1972). This depeneis on the individual's capacity to respond agression and its type (infection, toxic or mechanical effect as in the case of wide tympanic perforation).
We found areas with high population of ciliated cells even in mastoid, although we could see only a few in the promontory. Some ciliated cells presented cilia of dífferent length and some lost cilia (about these cells, it is not possible to assure if they act efficiently) (Friedmann I. & Bird E., 1981; Kawabata & Paparella M., 1969; Moller P. & Dallen H. 1981).
Basal cells were seen When there were loss of the superficial layer; they were fusiform in shape, resting on the basement membrane not only in ore layer but also in two or these lavers. Some of them were more cuboidal or polyhedral in shape and this probably due to the fact that they were in the transitory stage to intermediate cells (Hentzer E., 1970).
Loss of the superficial layer could be due to surgical trauma when the biopsy was taken. This is true when loss of superficial layer is limited to the margin of the specimens, but we found many arcas showing this change in the biopsy. On the other hand mucus druplets were seen on the surface of the remaining cells; but we are not sare if the mucus were secreted by these remaining cells or carne from the neighboring arcas.
In the inlammed mucosa of the upper respiratory tract, it is common to see loss of the epithelíum (Shimada T. & Lim J., 1972), which is replaced by the remaining basal cells. This occurs in normal as well as in pathological middle ear mucosa. The epithelia are renewed constantly and the extruded cells are replaced by new ones, which are derived from differentiation of basal cells (Lim J., 1976; Tos M.;1980).
It is a normal cycle of the cell that damaged cell fall down and is replaced. Under pathological condition such as infection, toxic, trauma, etc; this cycle becomes hyperactive and cell differentiation may be accelerated inorder to keep the balance (Tos M., 1980). This is the reason why we saw many arcas with great proliferation of secretory cells and other with extruded cells exposing underlying basal cells.
Loss of superficial layer was more frequently found in the promontory area. This is probably because the promontory is most likely exposed to trauma or infection.
Irregularly arranged or extruded cells and basal cells hyperplasia could be implicated by an active process of renovation of the epithelium (Tos M., 1980); the effect of proteolytic enzymes against cell junctions should also be considered (Reimer A. et. al., 1980).
Great proliferation of secretory cells were commonly seen in cases with mucoid effusion (Lim J. & Birck H., 1971; Moller P. & Dallen H., 1981); this high population of Secretory cells may be due to predominant differentiation of basal cells to non-ciliated cells at this stage of the disease. As pathological condition subsides, basal cell hyperplasia gradually decreases during several tumover cycles and cell type and its density become normal (Tos M., 1980).
There is no pathognomonic fmding in chronic otitis media. It depends on the stage of the disease, such as proliferative or degenerative.
REFERENCES
FRIEDMANN, I. & Bird E. Ciliary structure, Cliogenesis, Microvilli. (Electron Microscopy of the Upper Respiratory Tract). Laryngoscope 1852-1867, 1981.
HENTZER, E. Ultrastructure of the Normal Mucosa in the Human Middle Ear, Mastoid cavities and Eustachian tube. Ann. OtoL RhinoL LaryngoL 79, 1143, 1970. Ultrastructure of the Middle Ear Mucosa in Secretory Otitis Media. Acta Otolmyngologica 73: 394-401, 1972. Ultrastructure of the Middle Ear Mucosa. Ann. OtoL RhinoL LaryngoL 85 (Suppl: 25) 30, 1976.
KAWABATA,1`.'& Paparella M. Atypical Cilia in Normal Human and Guinea pig Middle Ear Mucosa. Acta Otolaryngologida 67: 511-515, 1969.
LIM, D. J.; Birck H. Ültrastructure Pathology of the Middle Ear Mucosa in Serous Otitis Media. Ann. Otol. 80: 838-853,1971.
LIM, D.J. Functional Morphology of the Mucosa of the Middle Ear and Eustachian tube. Ann. OtoL RhiwL LaryngoL 85 (Suppl 25) 36-43, 1976.
MOLLER, P. & DALLEN H.,Ultrastructure of the Middle Ear Mucosa in Secretory Otitis Media. Acta Otolaryngologica 91: 95-110, 1981.
REIMER,'A. et al. Mucociliary Activity of the Respiratory Tract. Acta Otolaryngologica 90: 462-469, 1980.
SHIMADA" T.,& LIMO D.IJ. Distribution of Cihated Cells in the Human Middle Ear. (Electron and Light Microscope observations~Ann. OtoL 81: 203-211, 1972.
TOS, M. Middle Ear Epithelia in Chronic Secretory Otitis. Arch.Otolaryngol. Vol. 106: 593-597, Oct. 1980.
1- Department of Otolaryngology. Hiroshima University School of Medicine.





Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial