|

| Código de la Imagen : 3674 | |
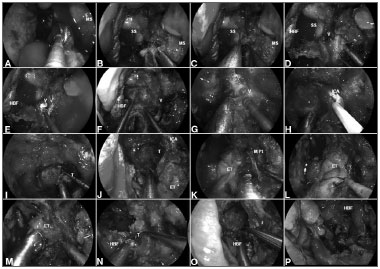
| Figure 4. A: Malignant clival tumor extending laterally beyond the paraclival ICA; therefore, requiring endoscopic transpterygoid. | |
Imagen publicada en: |
|
|
|
| 4 | |
| Descripción: | |
|
|
| Autor (es) del artículo de origen: | |
| Pornthep Kasemsiri; Daniel Monte Serrat Prevedello; Bradley Alan Otto; Matthew Old; Leo Ditzel Filho; Amin Bardai Kassam; Ricardo Luis Carrau | |
| Título y link del artículo: | |
| Endoscopic Endonasal endonasal technique: treatment of paranasal and anterior skull base malignancies | |
| oldfiles.bjorl.org/conteudo/acervo/acervo_english.asp?id=4531 |
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial