INTRODUCTIONThe important functions of the human larynx are the protection of lower airways and phonation. Unilateral vocal cord paralysis is the most common neurogenic disorder affecting the larynx.
1 Vocal fold paralysis occurs due to the involvement of the vagus or its recurrent laryngeal nerve between the jugular foramen and its entrance into larynx. 90% of paralyses are due to lesions affecting the nerves along their peripherally located segments. Only 15% are proximal to the jugular foramen.
2 The surgical treatment of choice in such cases is type I thyroplasty or medialization thyroplasty with or without arytenoid adduction. Based on the principles set forth by Isshiki, several modifications have been introduced. Over the years, the shape of silastic implants has been modified, and different materials have been used, such as Gore-tex and VoCom, among others. The titanium vocal fold medializing implant (TVFMI
®) is one of these modifications. This implant is intended to save time and provide good vocal cord medialization.
In this study, the voice improvements after type I thyroplasty using TVFMI
® and conventional Silastic
® implants were compared. The surgical time necessary and the costs of these implants were also assessed.
MATERIALS AND METHODSThis was a prospective study conducted in 40 patients with unilateral vocal cord paralysis at a tertiary care center after approval from the hospital's ethics committee (protocol approval No. -3/30, September of 2010).
The patients included in the study had unilateral vocal cord paralysis for more than six months and underwent type I thyroplasty with either Silastic
® implant or TVFMI
®. Revision thyroplasty and larynx malignancy cases were excluded from the study.
The patients of unilateral vocal cord paralysis were randomly divided into two groups to undergo type I thyroplasty using silastic implant and TVFMI
®. TVFMI
® is made by Gerhard Friedrich of Austria. It is produced by Heinz Kurz GmbH Medizintechnik Tuebinger Strasse 3 72144 Dusslingen, Germany. The implants used came from lot 2092720. Demographic data, including age and gender, were recorded, as well as the suspected etiology of the vocal cord paralysis. The patients then underwent a thorough general physical and ENT examination. The patients underwent objective assessment of voice using the voice handicap index (VHI), perceptual assessment of voice using GRBAS, videolaryngoscopy, and stroboscopic assessment of vocal cord function. Acoustic and electroglottographic voice assessments were also performed.
Videolaryngoscopic examination was performed along with stroboscopy (endostrobe with xenon light using 90 degree Hopkins laryngoscope). The examinations assessed the mobility of the cords, presence or absence of glottic gap at the time of adduction, and mucosal wave if present. The patients were given a VHI form to be completed by them. The voice of the patient was subjectively graded through the GRBAS scale and by a four-point Likert scale.
The patients also underwent voice analysis and electroglottography, which were performed using Dr. Speech software (Tiger DRS, Inc). The parameters considered for comparison in acoustic analysis (figure) were: maximum phonation time (MPT), fundamental frequency (F0), shimmer, jitter, harmonic to noise ratio (HNR), and normalized noise energy (NNE).
For EGG, the evaluated parameters were F0, jitter, shimmer, NNE, HNR, contact quotient (CQ), and contact quotient perturbation (CQP).
Following this analysis, the patients who qualified for surgery according to the treatment protocol (unilateral permanent RLN palsy with no improvement/compensation over six months) were considered for surgery. After the patients signed the informed consent, they underwent a standard type I thyroplasty with silastic implant (type B) (Fig. 1) or TVFMI
® (Fig. 2).

Figure 1 A, Carved-out type B silastic implant. B, Silastic implant placed in cartilage window.

Figure 2 A, Titanium vocal fold medializing implant (TVFMI
®). B, TVFMI
® placed in the cartilage window.
The extent of medialization was noted by asking the patient to vocalize and also by fiber-optic laryngoscopic examination to observe the position of the vocal cords. In cases of TVFMI
®, two types of implants were used: 15 mm for males and 13 mm for females.
The videolaryngoscopy, stroboscopy, VHI completion, GRBAS voice analysis, acoustic analysis, and electroglottography were performed both pre-operatively and at four weeks post-operatively. These parameters were recorded,- transferred into a MS Office Excel worksheet, and tabulated.
At the end of the study, the data were analysed using SPSS, version 17. Paired Student's t-test was used for comparing the pre- and post-operative VHI values. Pre- and post-operative values of GRBAS were compared separately using paired Student's t-test. Individual parameters of acoustic analysis and EGG were also compared pre- and post-operatively, and the p-values were calculated. Student's t-test for independent variables was used to compare the improvement in parameters (VHI, GRBAS, acoustic analysis, EGG) following the type I thyroplasty with silastic implant or TVFMI
®. p-values less than 0.05 were considered to be significant (95% confidence interval).
RESULTSThe study included 40 patients; 31 males (77%) and nine females (23%). The age and gender distribution of vocal cord paralysis varies according to the aetiology of the paralysis. In the present study, 26 patients were less than 50 years of age and 14 were over 50 years.
30 patients were of left vocal cord (75%) and 10 of right vocal cord (25%). The ratio of left to right vocal cord palsy is 3:1.
Out of these 40 patients, ten (25%) had a skull base/head and neck tumor. These tumors included glomus jugulare, vestibular schwannoma, and nasopharyngeal carcinoma. Five patients (12%) had developed vocal cord palsy following surgery (cardiothoracic); Four patients (10%) hade inflammatory pathologies (mediastinal lymphadenopathy, TB); and three patients (8%) had vocal cord palsy due to non-surgical trauma (fish bone injury, splinter injury). In the remaining 18 patients (45%), no cause could be identified, and they were said to have idiopathic vocal cord palsy.
Out of the 40 patients, 20 underwent type I thyroplasty with silastic implant and the remaining 20 with TVFMI
®.
Surgery duration varied according to the type of implant being inserted. In cases where conventional silastic implant was used, average surgery duration was 85.05 min. In cases where TVFMI
® was inserted, surgery duration was much shorter, 49.5 minutes.
Each TVFMI
® implant cost $330. In cases where TVFMI
® was inserted, an additional instrument, the moulding pliers, were required. They were a one-time investment of $215. The cost of the silastic block used in each surgery was $38.
Videolaryngoscopic and stroboscopic assessment demonstrated a reduction in glottic gap at the time of adduction in all cases except for one, with apposition of both vocal cords in the mid-line. There was only one case who underwent medialization with silastic implant and did not achieve complete closure of glottic gap. Mucosal wave pattern was not observed in any of the cases pre-operatively; post-operatively, it was present in 14 and 16 patients undergoing insertion of silastic implant and TVFMI
®, respectively.
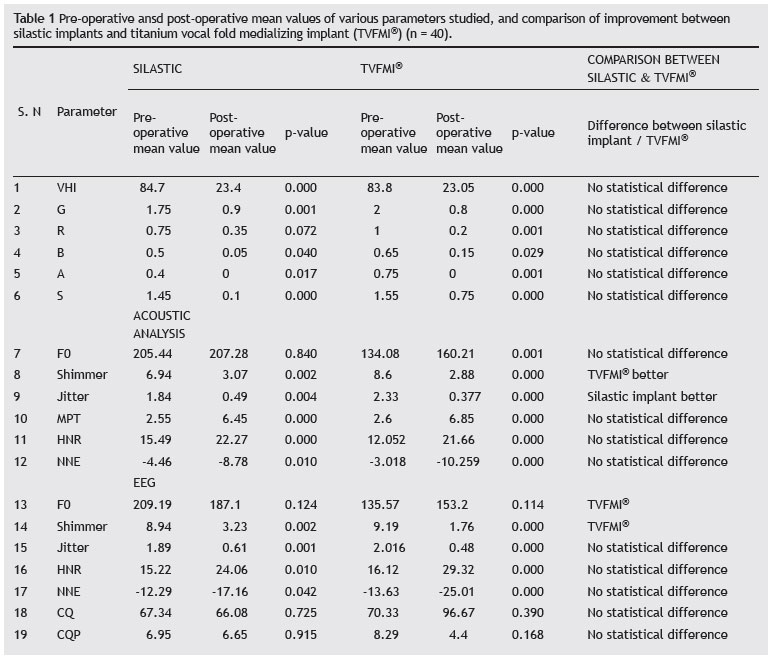
Table 1 shows the pre-operative and four weeks post-operative mean values of various parameters (VHI, GRBAS, acoustic analysism and electroglottography) studied and comparison of improvement between silastic implants and TVFMI
®.
DISCUSSIONUnilateral vocal cord paralysis is generally observed on left side, with the ratio of left to right ranging from 3 to 4:1.
2Unilateral vocal cord paralysis can present as hoarse voice, vocal fatigue, dysphagia, decreased pitch, decreased loudness, and aspiration. The severity of these symptoms depends on the position of the paralysed cord.
3 Various techniques have been developed to reduce the glottic gap, such as injection thyroplasty and medialization thyroplasty. Payr described an external medialization technique in 1915. In 1978, Isshiki revolutionized the surgical treatment for unilateral vocal cord paralysis by using silastic implant for medialization of the paralysed cord.
4,5 Based on the basic principles given by Isshiki, several modifications have been introduced. Over the years, the shape of silastic implant has been modified, and different materials were used, such as Gore-tex, Vo Com, and titanium, among others. Currently, individually-fitted implants based on computed tomographic (CT) images have been developed for use in medialization thyroplasty.
6 As in other studies,
2 the present study also observed that most of the cases were of unilateral vocal cord palsy; 25% were due to malignancies of head and neck, followed by surgical trauma, 12%. These are comparable to the documented percentages in other studies; patients with malignancies constitute 25% of the cases with unilateral vocal cord palsy, the same as that of the present study. Non-surgical trauma has been shown to contribute 15% of the cases, which is also similar to the present study. Literature reports inflammatory causes as responsible for 5% of cases; in the present study, this rate was 10%. This was perhaps due to the higher number of chronic infective diseases observed in the Indian study. 8% of patients were of non-surgical trauma in the present study. In 45%, no cause could be identified, and they were labelled as idiopathic; this high percentage could again be due to higher number of infective (viral) pathologies in the present study.
The average surgery duration was 85.05 minutes for silastic implant and 49.5 minutes for TVFMI
®. One study reported surgery durations of 65 minutes for silastic implant and 55 minutes for TVFMI
®.
7 Other studies also reported shorter surgery times for TVFMI
®. TVFMI
® is pre-moulded, so that only its posterior limb needs to be adjusted, and it has been shown to be easier to insert and fix, thus reducing the operative time.
5,7-10 The present study used time compared to other studies in cases where silastic implant was inserted, because the silastic implant was moulded at the time of surgery. Keeping the silastic block pre-moulded may reduce the surgical time, as observed in other studies. TVFMI
® is costlier than silastic implant and also requires a specialized tool (bending pliers) for insertion.
The improvement in quality of life scales, such as VHI, was observed in various studies.
6,9 In the present study, a statistically significant post-operative improvement in VHI was observed with both silastic implant and TVFMI
®. No statistically significant difference was observed between the improvements in the score of the two implants. Several studies have found the improvement in VHI to be a good indicator of voice improvement.
11GRBAS is a well-known scale for perceptual assessment of voice.
12 The voice of the patients improved post-operatively, but it was still not normal. Perceptual analysis by GRBAS scale showed improvement. Breathiness, asthenia, and strain in voice were reduced, but roughness persisted post-operatively. Improvement in mean roughness score in patients treated with silastic implant was not found to be significant. Overall, the voice grading improved with surgery. Other studies
7,9,10 have shown similar improvement in the perceptual scores post-operatively, even though the voice may still be rough and hoarse.
Endoscopic evaluation of vocal cord movement is an important tool.
13 On videolaryngoscopic and stroboscopic examination, the glottic gap was found to be reduced in all but one case who underwent type I thyroplasty with silastic implant. This was a case of idiopathic vocal cord palsy. During intra-operative fibreoptic laryngoscopic assessment, the glottic closure was found to be adequate; however, at follow-up, vocal cord atrophy was observed and the glottic gap reappeared. Mucosal wave pattern was not observed in any of the cases pre-operatively; post-operatively, it was present in 14 and 16 patients undergoing insertion of silastic implant and TVFMI
®, respectively. Due to better glottic closure, the patients had a better voice quality and could also cough more effectively. Glottic gap closure was found to be reduced in 93% to 100% of cases following type I thyroplasty.
7,10 Storck et al. observed that TVFMI
® pushes the entire cord medially, and hence gives better results.
In the acoustic analysis and electroglottography, shimmer and jitter were reduced; maximum phonation time increased substantially, allowing patients to speak without voice breaks. HNR and NNE also improved, thus the hoarseness of voice decreased. There was improvement in the contact quotient of the vocal cords, and its perturbation decreased. The overall result was improved voice quality, as observed in several other studies.
7-10 Jitter and shimmer percentage have been reported to improve after TVFMI
® insertion from 7.15 to 3.58 and from 27.8 to 13.69, respectively.
8 Other studies have also observed statistically significant improvements in jitter and shimmer .
On objective testing, TVFMI
® presented superior results to silastic implant regarding to the following parameters: shimmer (acoustic and EGG) and F0 (EGG). Considering all the parameters, TVFMI
® was better than silastic implant in only three. Better outcome with TVFMI
® in these objective parameters may have been due to the case who had inadequate glottic closure with silastic implant. In VHI, perceptual rating of voice with GRBAS, and acoustic analysis and electroglottography, the voice improvement was statistically similar with both types of implants. The medialization of vocal cords was adequate in both types of implants, and the glottic gap was adequately reduced in both. Other studieshave observed that TVFMI
® presented a better voice outcome and shorter surgical duration.
7-10 In the present study, the voice outcomes were similar between TVFMI
® and silastic implant, except for the few abovementioned objective parameters. The case that presented inadequate glottic closure with silastic implant may have been responsible for a slight bias in objective parameters towards TVFMI
®.
CONCLUSIONThis study has demonstrated that, in cases of unilateral vocal cord palsy, there is a subjective improvement following type I thyroplasty using both silastic and TVFMI
® implants (VHI and GRBAS). Videolaryngoscopy and stroboscopy demonstrated a reduction in glottic gap in all cases but one after surgery. TVFMI
® presented slightly better result in objective voice analysis, but the impact of the case with persistant glottic gap after medialization with silastic implant should be taken into consideration. Type I thyroplasty with TVFMI
® is faster, but more expensive.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.
REFERENCES1. Woodson GE. Laryngeal and Pharyngeal function. In: Flint PW, Haughey BH, Niparko JK, Richardson MA, Robbind KT, Thomas JR, eds. Cummings Otolaryngology Head & Neck Surgery. 5
th ed, Vol 1. Philadelphia: Mosby Elsevier; 2010. p. 805-12.
2. Rehabilitation of speech and swallowing. Watkinson JC, Gaze MN, Wilson JA, editors. Stell & Maran's head & neck surgery. 4th edition. London: Hodder Arnold; 2007. p.357-376.
3. Woodson G. Evolving concepts of laryngeal paralysis. J Laryngol Otol. 2008;122:437-41.
4. Friedrich G. Titanium vocal fold medializing implant: introducing a novel implant system for external vocal fold medialization. Ann Otol Rhinol Laryngol. 1999;108:79-86.
5. Isshiki N, Morita H, Okamura H, Hiromoto M. Thyroplasty as a new phonosurgical technique. Acta Otolaryngology. 1974;78:451-7.
6. Frizzarini R, Gebrim EM, Imamura R, Tsuji DH, Moyses RA, Sennes LU. Individually customized implants for laryngoplasty - are they possible? J Voice. 2012;26:619-22.
7. Storck C, Fischer C, Ceco M, Schmid S, Gambazzi F, Wolfensberger M, et al. Hydroxyapatite versus titanium implant: comparison of the functional outcome after vocal fold medialization in unilateral recurrent nerve paralysis. Head Neck. 2010;32:1605-12.
8. Witt RE, Hoffman MR, Friedrich G, Rieves AL, Schoepke BJ, Jiang JJ. Multiparameter analysis of titanium vocal fold medializing implant in an excised larynx model. Ann Otol Rhinol Laryngol. 2010;119:125-32.
9. Schneider B, Denk D, Bigenzahn W. Acoustic assessment of the voice quality before and after medialization thyroplasty using titanium vocal fold medialization implant (TVFMI). Otolaryngol Head Neck Surg. 2003;128:815-22.
10. Schneider B, Denk D, Bigenzahn W. Functional results after external vocal fold medialization thyroplasty with the titanium vocal fold medialization implant. Laryngoscope. 2003;113:628-34.
11. Jacobson BH, Johnson A, Grywalski C, Silbergleit A, Benninger MS. The voice handicap index (VHI): development and validation. Am J Speech Lang Path. 1997;6:66-70.
12. Titze IR. Workshop on Acoustic voice analysis: summary statement. Iowa City, IA: National Centre for Voice and Speech;1995.
13. Hirano M, Bless DM. Videostroboscopic examination of the larynx. London: Whurr Publishers Ltd; 1993.
Department of Otorhinolaryngology, Army Hospital (R&R), Delhi Cantt, India
Corresponding author.
A. Malik
E-mail:
akshatmalik@gmail.comReceived 12 July 2013.
Accepted 10 November 2013.