INTRODUCTIONSubglottic hemangioma is one of the most common airway vascular neoplasms in children. It usually presents with inspiratory or biphasic stridor, increased by feeding and upper airway infections1. During its proliferative stage, usually before 12 months of age, it can be fatal if diagnosis and treatment are not started quickly2.
Surgical treatment is based on tracheostomy, surgical excision of the lesion, local injection of steroids and laser2. Recently, several authors have proposed a clinical management with propranolol, yielding good results3. The goal of the present study was to describe an infant with inspiratory stridor developed after hospitalization for acute viral bronchiolitis, with a final diagnosis of subglottic hemangioma and indication of clinical treatment.
CASE REPORTAn eight month-old female, with a history of stridor perceived by the mother, especially during sleep. She was hospitalized at four months of age because of an acute viral bronchiolitis (without findings of respiratory viruses). She required supplemental oxygen for three days and symptomatic medication. She was breastfed only until the fourth month without significant perinatal history. She had normal PKU test, proper weight and height gains, and had been properly vaccinated. The mother reported stridor improvements with oral steroids.
Upon physical examination, the infant was eutrophic, with mild inspiratory stridor; and rare transmission snoring upon pulmonary auscultation. A high resolution chest CT scan associated with virtual bronchoscopy showed a vascular lesion in the subglottis, blocking about 90% of the airway (Figure 1). The proposed treatment was propranolol (2mg/kg/day) associated with prednisolone (1mg/kg).
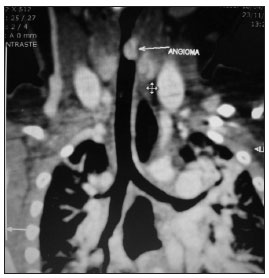
Figure 1. Chest and neck CT scan showing an angioma
Stridor in infants may be translated into a wide range of conditions, some of them potentially life-threatening, such as subglottic hemangioma with airway obstruction. As congenital causes, we list: laryngomalacia, subglottic stenosis, vocal cord paralysis, laryngocele and laryngeal membranes. The main acquired causes are foreign body aspiration, hemangiomas, recurrent papillomatosis and croup4. Hemangiomas may spontaneously regress later on, by 5 years of age.
Until recently, the best treatment for this type of condition was surgery, with reports of up to 94.5% of success in some series. However, because of the rich vascularization of the lesion and its anatomical location, the risks inherent to the procedure should not be disregarded. Thus, the use of clinical treatment represents an important advance for this condition.
Monotherapy with oral steroids may fail in up to 75% of the patients, and it has its side effets6. Beta-blockers, such as propranolol, may represent an inexpensive alternative, which is also non-invasive and well-tolerated by the patient4; not forgetting the paramount need for a cardiological assessment of the patient (echocardiogram and electrocardiogram) before treatment onset. The mechanism of action involved is related to the inhibition of mitogenic factors stimulating apoptosis in capillary endothelial cells. The aforementioned patient has been asymptomatic after one month of therapy, and will soon be off the steroids.
FINAL REMARKSTreatment with propranolol is inexpensive, noninvasive and well tolerated, it may prevent the patient from being submitted to surgery or event tracheostomy because of disease progress. Such medication can cause bradycardia, decreased blood pressure and hypoglycemia. The authors' recommendation is that once the subglottic hemangioma is diagnosed in children, propranolol is a valuable tool for treatment, pending a paramount cardiac evaluation prior to the start of medication.
REFERENCES1. Blanchet C, Nicollas R, Bigorre M, Amedro P, Mondain M. Management of infantile subglottic hemangioma: acebutolol or propranolol? Int J Pediatr Otorhinolaryngol. 2010;74(8):959-61.
2. Bitar MA, Moukarbel RV, Zalzal GH. Management of congenital subglottic hemangioma: trends and success over the past 17 years. Otolaryngol Head Neck Surg. 2005;132(2):226-31.
3. Denovelle F, Leboulanger N, Enjolras O, Harris R, Roger G, Garabedian EN. Role of Propranolol in the therapeutic strategy of infantile laryngotracheal hemangioma. Int J Pediatr Otorhinolaryngol. 2009;73(8):1168-72.
4. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, Boralevi F, Thambo JB, Taïeb A.. Propranolol for severe hemangiomas of infancy. N Engl J Med. 2008;358(24):2649-51.
5. Saetti R, Silvestrini M, Cutrone C, Narne S. Treatment of congenital subglottic hemangiomas: our experience compared with reports in the literature. Arch Otolaryngol Head Neck Surg. 2008;134(8):848-51.
6. Jephson CG, Manunza F, Syed S, Mills NA, Harper J, Hartley BE. Successful treatment of isolated subglottic haemangioma with propranolol alone. Int J Pediatr Otorhinolaryngol. 2009;73(12):1821-3.
1. MD. MSc.
2. MD. Pediatric Pneumologist.
3. MD. Radiologist.
4. MD. Chest Surgeon - Hospital Municipal São José, Joinville.
Send correspondence to:
Hospital Infantil Jeser Amarante Faria
Rua Três Barras, 539, casa 01, Bairro Saguaçu
Joinville-SC.
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on December 15, 2010.
Accepted on March 07, 2011. cod. 7471
