INTRODUCTIONStudies in the past 15 years have shown that the cochlear implant is an effective treatment for profound hearing loss in infants. Early restoration of auditory implant by cochlear implants significantly improve the communication skills, albeit with varied results1,2. While most children with cochlear implants become able to attend school regularly, other remain with significantly limited verbal communication skills3.
It is known that the efficacy of cochlear implants depends on several factors. Many studies have searched for factors that improve the results. Duration of sensory deprivation, general development potential, possible concurrent conditions, age at surgery, anatomical/physiological and technological factors, and family involvement are examples of reported variables affecting the efficacy of cochlear implants4-7.
Most studies on the impact of cochlear implants have focused on clinical assessments of efficacy (hearing and speech skills, and auditory thresholds). However, these measures are only part of the effect of cochlear implant treatment. Because of the major impact of deafness on communication, it is not clear how much clinical measures of efficacy (for instance, speech, hearing, and language measures) truly show the effectiveness of cochlear implants in general contexts (such as performance at home, at school, and in social settings). Single texts do not assess the ability of children to communicate their needs and wishes, or any improvement in self-confidence among children when interacting with normal hearing colleagues. There is evidence that clinical assessment results do not correlate with performance in unstructured settings8.
Because communication skills and social life often change after a cochlear implant is placed, its efficacy should be assessed taking into account structure evaluation tests and instruments for assessing the ease of daily communication, social relations, well-being, and other components of quality of life9,10.
A need to measure results more widely has stimulated an interest in using quality of life measures for assessing the impact of cochlear implants. Thus, generic multidimensional health tools to assess the quality of life of populations at large have been widely used. These tools are not necessarily sensitive enough in audiological evaluations or to assess the results of rehabilitation, as they do not detect clinically significant improvements in users of cochlear implants11,12. The potential psychosocial benefits of using cochlear implants - such as well-being and measures of health status - are not measured in these generic instruments13.
Open and closed question interviews and questionnaires or semi-structured questionnaires usually are more informative for monitoring purposes after cochlear implant surgery than generic instruments. Specific questionnaires for cochlear implant users yield information about real life situations and help describe the child's activities and participation in various social ambiences. Thus, a valid study should use adequate tools for assessing the relevant quality of life issues in the target population.
Besides being excellent research tools, questionnaires are widely used for control and quality assurance purposes in clinical settings, irrespective of interviewees - whether patients or caretakers for pediatric groups. Questionnaires help standardize information about perceptions that parents and caretakers have about implants, and inform teaching and healthcare professionals.
There are few studies in the international literature on interviews and questionnaires that investigate the expectations of parents1-3,8,14-16, their satisfaction level with implant placement14,15, the stresses in this process8, and cochlear implant user and family quality of life8,14.
The Children with Cochlear Implants: Parent´s Perspectives (CCIPP), developed by Archbold et al.17, is one of the most frequently used questionnaires for evaluating the quality of life in children with cochlear implants. The CCIPP is used worldwide in many cochlear implant centers (Ear Foundation, 2009) and has been described as an excellent research and clinical tool17,18. It is a validated and reliable questionnaire that is applied when studying the experience and opinions of parents about several aspects of the quality of life of children and their families following cochlear implant surgery19-21.
Because of different cultures and healthcare system, changes in quality of life after cochlear implant surgery need to be studied according to cultural contexts and communication approaches. It is, therefore, extremely important to apply validated tools developed specifically for Brazilian children using cochlear implants, to assess their quality of life. Thus, the purposes of this study were:
1 - To translate and adapt the questionnaire Children with cochlear implants: parental perspectives (Ear Foundation) into Brazilian Portuguese.
2 - To apply the questionnaire to parents of children using cochlear implants and to investigate the quality of life of children and their families after cochlear implants are placed.
3 - To analyze possible correlations among factors relating to the experience and expectations of parents on the quality of life of children and the family.
4 - To analyze possible correlations among experiences and expectations of parents about the quality of life and the results of cochlear implants.
METHODS
Ethical issuesThe institutional review board approved the study and the free informed consent form (protocol no. 342/10). All caretakers voluntarily signed the free informed consent form after agreeing to participate in the study.
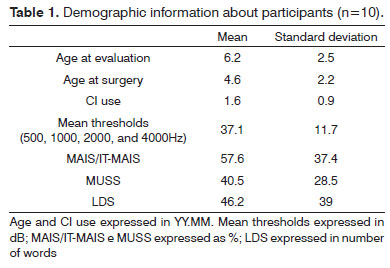
SubjectsThe study sample comprised 10 infants (five male and five female) that had cochlear implants (mean age - 6 years and 2 months; standard deviation - 2.5) and their parents or caretakers. The following criteria were applied to select the sample:
1. At the time data were gathered, participants should be attending speech therapy.
2. Participants should be infants (aged from 4 to 8 years).
3. Participants should have no medical conditions or concomitant factors, such as loss of vision or compromised motor development.
4. Participants should present pre-language deafness.
Table 1 shows additional participant data.
MATERIALParents or caretakers of participants answered the following instruments:
Children with cochlear implants: parental perspectives (CCIPP)17.The CCIPP questionnaire consists of 74 statements with multiple choice answers in a Likert 5-point scale: agree completely (coded 5), agree (4), neither agree nor disagree (3), disagree (2), and disagree completely (1). Forty-six statements in this questionnaire are written in a positive format and 28 are written in a negative format.
In total, 40 questions are analyzed quantitatively in subscales (general questions) consisting of three to six items. Subscale topics on child's status are: communication, general function, self-sufficiency, well-being and happiness, social relationships, and education. Subscale topics on family are: effects of the implant, and support to the child. Higher scores indicate a more positive parent perspective.
Language Development Survey22 (Lista de Avaliação Vocabulário Expressivo, or LAVE) adapted into Brazilian Portuguese by Capovilla & Capovilla23.Studies have shown that the word repertoire acquisition is delayed in children with profound hearing loss compared to normal hearing children of similar age10,18,24,25. One of the reasons for this is that an anatomically and physiologically intact auditory system is a prerequisite for language acquisition and development, and its absence results in poor lexical development. Family interventions are another fundamental factor in language development; language performance in children is positively influenced by family involvement and the mother-child interactions - the linguistic input from the family, which defines the child's lexicon.
The Language Development Survey (LDS)22,26 is frequently used to check lexical development. It comprises a checklist of words, to be filled in by parents. Capovilla & Capovilla23 published a translated and adapted version of the LDS in Portuguese - the name given to the test was "Lista de Avaliação de Vocabulário Expressivo or LAVE". Although the survey is widely used, only a single study on its use in Brazilian children using cochlear implants was found27.
Meaningful Use of Speech Scale (MUSS)28,29The Meaningful Use of Speech Scale (MUSS) questionnaire was used to analyze and measure speech skills. Nascimento29 translated and adapted the MUSS into Brazilian Portuguese. It consists of a structured interview of parents to assess speech use in daily situations. As with the MAIS and the IT-MAIS, the MUSS comprises 10 questions to evaluate the following areas: 1) voice control; 2) using speech without gestures or signs; and 3) using communication strategies in daily situations. Specific scoring criteria are applied to each question. The general score is obtained by adding the scores for each area.
Meaningful Auditory Integration Scale (MAIS)28,29 or The Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS)29,30Auditory skills were measured and analyzed by the Meaningful Auditory Integration Scale (MAIS) or Infant-Toddler Meaningful Auditory Integration Scale (IT-MAIS)30 questionnaires, according to the child's age. Both consist of structured interviews to assess the spontaneous responses of children to sounds in their daily living environments. Castiquini & Bevilaqua31 translated and validated the MAIS and IT-MAIS questionnaires into Brazilian Portuguese.
The assessment is based on information provided by parents to ten questions about three areas: 1) vocalization behavior; 2) alert to sounds; and 3) meaning of sounds. Specific scoring criteria are applied to each question. The general score is obtained by adding the scores for each area.
Data analysisQuantitative data were analyzed using the SPSS version 16 software. The adopted statistical significance was
p<0.05. The descriptive analysis consisted of minimum and maximum measures, means, and quartiles, presented as box plots. Inferential analysis was done using a non-parametric measure of statistical dependence between two variables (Spearman's rho).
RESULTSObjective 1: To translate and adapt the CCIPP17 questionnaire into Brazilian PortugueseThe Ear Foundation, UK, authorized the translation and adaptation into Brazilian Portuguese of the questionnaire CCIPP (in Portuguese, "
Crianças com Implante Coclear: Perspectivas dos Pais"), according to the norms of the EORTC Quality of Life Study Group: Translation Procedure32.
At first, two speech therapist that were native Brazilian Portuguese speakers and fluent in English undertook two translations and cultural adaptations of the CCIPP questionnaire into Brazilian Portuguese. After comparing the two translations, both speech therapists generated a single Brazilian Portuguese version.
The final version of the questionnaire is annexed to this paper (Annex 1: CCIPP,
Crianças com Implante Coclear: Perspectiva dos Pais - girls; Annex 2: CCIPP,
Crianças com Implante Coclear: Perspectiva dos Pais - boys).
Objective 2: To analyze the quality of life of children and their families after implanting cochlear implantsOn average, use of cochlear implants improved the quality of life of children and their families in all aspects of CCIPP subscales according to the parents (Figure 1).
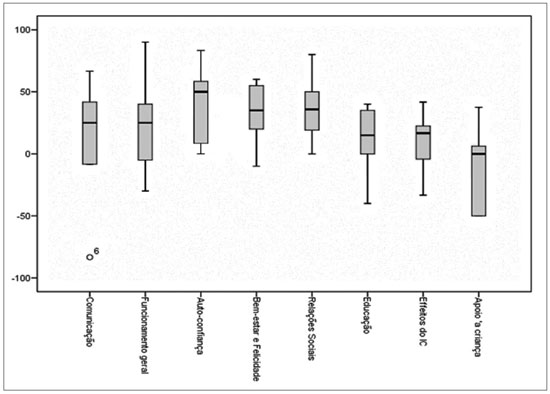
Figure 1. Mean values of the perception of parents in the subscales of the "Crianças com Implante Coclear: Perspectivas dos Pais" questionnaire, represented as box plots. Higher means correlate with more positive parent's perspectives.
Expectations of parents were more satisfactory on child self-confidence and well-being.
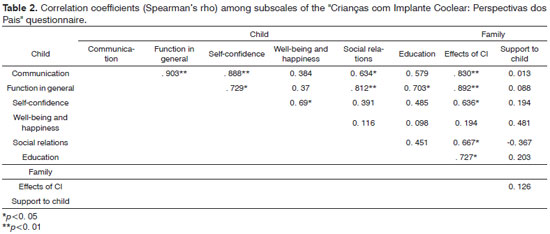
Objective 3: To analyze possible correlations among CCIPP subscalesStatistically significant correlations among CCIPP subscales were found (Table 2). The largest number of correlations was found in the communication subscale - a direct relationship between communication and other quality of life variables.
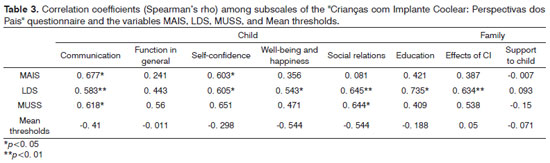
Objective 4: To analyze possible correlations among CCIPP subscales and the results of cochlear implantsTable 3 shows the correlations among CCIPP subscales and the results of placing cochlear implants. Lexical development skills (in the LDS), auditory skills (in the MAIS/IT-MAIS), and speech skills (in the MUSS) are significantly related with the communication subscale of the CCIPP from the perspective of parents.
Fewer significant correlations were seen in the development of auditory (MAIS/IT-MAIS) and speech (MUSS) skills compared to lexical development.
DISCUSSIONThe purpose of this study was to present the CCIPP questionnaire in a translated and culturally adapted version in Brazilian Portuguese. It also aimed at analyzing the quality of life of children and their families and to assess possible correlations among quality of life factors and communication skills after cochlear implants were placed.
Standardizing instruments for several countries makes it easier to compare findings across populations, which adds external validity to studies and increases knowledge on a given topic. Our results are a contribution in this direction by a translation and adaptation of the CCIPP questionnaire into Brazilian Portuguese (see Annexes). This translated questionnaire is referenced worldwide.
An analysis of Brazilian children using cochlear implants showed that parents perceive a significant effect of these implants on the quality of life of children and their families. On average, one positive effect of cochlear implants was found in all aspects of the CCIPP subscale. Parents were more satisfied with self-confidence, social relationships, well-being, happiness, general function, and communication of children. These findings corroborate those of a previous study10 on the five areas reported as the most satisfactory by parents after cochlear implants were placed.
In the international literature, improved self-confidence and social relationships are the earliest reported benefits of cochlear implants33,34. Our results concur with these findings. Parental expectations in Brazil were met mostly in self-confidence, social relationships, and child well-being.
We found statistically significant correlations between several CCIPP subscales (Table 2). More correlations were found in the communication and implant effects subscales. Our findings show that parents find a directly relationship between communication and other quality of life variables - effects of cochlear implants, social relationships, self-confidence, and function in general. Additionally, these associations mean that better communication correlates with increased independence in children (better self-confidence) and improved interactions between the child and friends and family members (social relationships). The implant effect is associated with improved oral communication, more self-confidence, increased well-being and happiness, better social relationships, and a positive effect on education.
In contrast, the child support subscale did not correlate with any other subscale, meaning probably that the family supports their children irrespective of the results in other areas evaluated in this study.
From the parent's perspectives, lexical development skills (in the LDS), auditory skills (in the MAIS/IT-MAIS), and speech skills (in the MUSS) had a significant influence on the communication subscale of the CCIPP. This finding demonstrates that these instruments are mutually compatible and reinforces the validity of the Brazilian Portuguese version of the CCIPP.
Auditory thresholds were not associated with any of the quality of life subscales in this study. There were more significant correlations in lexical development skills (in the LDS) compared to development of auditory skills (in the MAIS/IT-MAIS) and speech skills (in the MUSS). Fewer relationships in auditory thresholds, and speech and auditory skill measures suggest a direct non-relation between these skills and improved quality of life, from the perspective of parents. A possible reason is that these are clinical measures and therefore not directly perceived by non-experts - the parents, for instance.
Lexical development data (in the LDS) were similar to the parent's opinions about the child's development in communication, self-confidence, well-being and happiness, social relationships, education, and effects of cochlear implants. Statistically significant correlations were found by comparing the results of LDS and the scores in each of these subscales (Table 3). These findings underline the value parents attribute to lexical development in children; our data suggest that for parents, development of a lexicon is the most closely related factor with the positive effects on the quality of life of their children.
The translated and adapted version of the CCIPP that is presented in this study was shown to be a valid instrument for use in the Brazilian pediatric population with cochlear implants. Satisfactory results were encountered, and it was compatible with other widely used instruments in this population group (such as the MAIS, IT-MAIS, and MUSS). The CCIPP provides a systematic form of investigating quality of life issues related with cochlear implant use by individuals and groups. Our proposed translation and adaptation may be applied by cochlear implant teams that intend to monitor the general effects of these devices. Individual results may yield a baseline for talks with parents, and group results can raise topics for debates among cochlear implant teams. Satisfactory results and areas of concern may be highlighted and taken into account in planning the goals of the team.
CONCLUSIONTranslation and cultural adaptation of the CCIPP questionnaire17 was satisfactorily concluded; this paper makes the CCIPP available in Brazilian Portuguese.
In the present study, cochlear implants had a positive effect on the lives of child users and their families. The correlations in the communication variable show a direct relationship between oral communication and quality of life.
Development of lexical, auditory, and speech activities were significantly related with the communication variable and quality of life. However, for parents of Brazilian child user of cochlear implants, quality of life aspects appear to be related more with lexical development than other communication skills that were evaluated in this study.
REFERENCES1. Tomblin JB, Spencer L, Flock S, Tyler R, Gantz B. A comparison of language achievement in children with cochlear implants and children using hearing aids. J Speech Lang Hear Res. 1997;42(2):497-509.
2. Svirsky MA, Teoh SW, Neuburger H. Development of language and speech perception in congenitally, profoundly deaf children as a function of age at cochlear implantation, Audiol Neurootol. 2004;9(4):224-33.
3. Thoutenhoofd E, Archbold S, Gregory S, Lutman ME, Nikolopoulos TP, Sach T. Paediatric cochlear implantation: evaluating outcomes. Elsevier; 2005.
4. Miranda C. Language Disorders in Children with hearing Impairment. In: Handbook of Child Language Disorders. Schwartz RG (Ed). New York: Psychology Press; 2008.
5. Schorr EA, Roth Froma P, Fox NA. A Comparison of the Speech and Language Skills of Children with Cochlear Implants and Children With Normal Hearing. Communication Disorders Quarterly. 2008;29(4):195-210.
6. Ertmer DJ, Strong LM, Sadagopan N. Beginning to communicate after cochlear implantation: oral language development in a young child. J Speech Lang. Hear Res. 2003;46(2):328-9.
7. Miyamoto RT, Hay-Mccutcheon MJ, Kirk KI, Houston DM, Bergeson-Dana T. Language skills of profoundly deaf children who received cochlear implants under12 months of age: a preliminary study. Acta Oto-Laryngologica. 2008;128(4):373-7.
8. Vidas S, Hassan R, Parnes LS. Real-life performance considerations of four pediatric multi-channel cochlear implant recipients. J Otolaryngol. 1992;21(6):387-93.
9. Nikolopoulos H, Lloyd SM, Archbold GM. O'Donoghue. Pediatric cochlear implantation: the parent's perspective. Arch Otolaryngol Head Neck Surg. 2001;127(4):363-7.
10. Huttunen M, Sorri T, Välimaa. Parents' views of their children's ha¬bilitation after cochlear implantation. In: Measuring the Immeasurable? Proceedings of a Conference on Quality of Life in Deaf Children, Nottingham. Oxford: Hughes Associates; 2003.
11. Holt J. Classroom attributes and achievement test scores for deaf and hard of hearing students. Am Ann Deaf. 1994;139(4):430-7.
12. Carney AE, Moeller MP. Treatment efficacy: hearing loss in children. J Speech Lang Hear Res. 1998;41(1):S61-84.
13. Schilling LS, DeJesus E. Developmental issues in deaf children. J Pediatr Health Care. 1993;7(4):161-6.
14. Marschark M. Origins and interactions in the social, cognitive, and language development of deaf children. In: Marschark M, Clark D (Eds.). Psychological Perspectiveson Deafness, Lawrence Erlbaum Associates. New Jersey: Hillsdale; 1993.
15. Vaccari C, Marschark M. Communication between parents and deaf children: implications for social-emotional development. J Child Psychol Psychiatry. 1997;38(7):793-801.
16. Spilker B, Revicki D. Taxonomy of Quality of Life. In: Quality of Life and Pharmaco economics in Clinical Trials. Spilker B (Ed.). Baltimore: Lippincott Williams & Wilkins; 1996.
17. Archbold M, Lutman S, Gregory C, O'Neill T, Nikolopoulos. Parents and their deaf child: their perceptions three years after cochlear implantation. Deaf Educ Int. 2002;4(1):12-40.
18. Archbold T, Nunes M, Lutman U, Pretzlik S, Gregory. Parental perspec¬tives of children with cochlear implants: the validated questionnaire. In: Measuring the Immeasurable? Proceedings of a Conference on Quality of Life in Deaf Children. Oxford: Hughes Associates; 2003.
19. Nunes U, Pretzlik. An independent Assessment and Evaluation of a Profile from Parents of Deaf Children with a Cochlear Implant. Oxford: Oxford Brookes University; 2003.
20. O'Neill M, Lutman S, Archbold S, Gregory T, Nikolopoulos. Parents and their cochlear implanted child: questionnaire development to assess parental views and experiences. Int. J Pediatr Otorhinolaryngol. 2004;68(2):149-60.
21. Nunes T, Pretzlik U, Ilicak S. Validation of a parent outcome questionnaire from a pediatric cochlear implantation. J. Deaf Stud Deaf Educ. 2005;10(4):330-56.
22. Rescorla L, Alley A. Validation of the language development survey (LDS): a parent report tool for identifying language delay in toddlers. J Speech Lang Hear Res. 2001;44(2):434-5.
23. Capovilla FC, Capovilla AGS. Desenvolvimento Lingüístico na Criança dos Dois aos Seis Anos: Tradução e Estandardização do Peabody Picture Vocabulary Test de Dunn & Dunn, e da Language Development Survey de Rescorla. Ciência Cognitiva: Teoria, Pesquisa e Aplicação. 1997;1(1):353-80.
24. Sach T. Current knowledge and future directions: the economics of cochlear implantation. In: Cochlear Implantation: Cost Creating or Cost Saving? Proceedings of Conference on Health Technology Assessment, Queen's Medical Centre. Oxford: Hughes Associates; 2002.
25. Purdy SC, Chard LL, Moran CA, Hodgson SA. Outcomes of cochlear implants for New Zealand children and their families. Ann Otol Rhinol Laryngol Suppl. 1995;166:102-5.
26. Rescorla L, Achenbach T. Use of the language development survey (LDS) in a national probability sample of children 18 to 35 months old. J Speech Lang Hear Res. 2002;45(4):733-43.
27. Mota JM, Fortunato-Tavares T, Koji RT, Bento RF, Matas CG, Andrade CRF, et al. Efeito do Programa de Orientação a Pais no Desenvolvimento Lexical de Crianças Usuárias de Implante Coclear. Arq Int Otorrinolaringol. 2011;15(1):54-8.
28. Robbins AM, Osberger MJ. Meaningful Use of Speech Scale (MUSS). Indianapolis: Indiana University School of Medicine;1990.
29. Nascimento LT. Uma Proposta de Avaliação da Linguagem Oral (Monografia). Hospital de Pesquisa e Reabilitação de Lesões Lábio-Palatais. 1997.
30. Zimmerman-Phillips S, Robbins AM, Osberger MJ. Infant-Toddler Meaningful Auditory Integration Scale. Sylmar: Advanced Bionics Corp; 2001.
31. Castiquini EAT, Bevilacqua MC. Escala de Integração Auditiva Significativa: Procedimento Adaptado para a Avaliação da Percepção da Fala. Rev Soc Bras Fonoaudiol. 2000;6(1):51-60.
32. Cull A, et al. EORTC Quality of Life Study Group: Translation Procedure. Brussels: EORTC; 2002.
33. Kelsay DMR, Tyler RS. Advantages and disadvantages expected and realized by pediatric cochlear implant recipients as reported by parents. Am J Otol. 1996;17(6):866-73.
34. Kluwin TN, Stewart DA. Cochlear implants for younger children: a preliminary description of the parental decision process and outcomes. Am Ann Deaf. 2000;145(1):26-32.
1. Speech therapist, doctoral student in human communication-rehabilitation science, Medical School, Sao Paulo University.
2. Speech therapist, associate professor of the Speech Therapy Course, Physical Therapy, Speech Therapy, & Occupational Therapy Department, Medical School, Sao Paulo University.
3. Otorhinolaryngologist, full professor of otorhinolaryngology, Medical School, Sao Paulo University.
4. Speech therapist, full professor of the Speech Therapy Course, Physical Therapy, Speech Therapy, & Occupational Therapy Department, Medical School, Sao Paulo University.
Central Institute of the Clinic Hospital, Medical School, Sao Paulo University (Instituto Central do Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo).
Send correspondence to:
Talita Fortunato-Tavares
Rua Cipotânea, 51, Cidade Universitária - Butantã
São Paulo - SP. CEP: 05360-160.
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on February 18, 2011.
Accepted on July 14, 2011. cod. 7585.