INTRODUCTIONAudiologic diagnosis within the first few weeks or months of life has become more frequent with neonatal screening programs1. Accurate information about the type, grade, and configuration of hearing loss is required for early audiological interventions to be successful.
Electroacoustic and electrophysiologic tests, in particular otoacoustic emissions (OAE) and the auditory brainstem response (ABR), are recommended for defining the behavioral audiogram in children aged below 6 months2.
The ABR with clicks is commonly used in children. Although less used in clinical settings due to increased testing time, tone burst stimuli are very useful because it is frequency specific, and therefore can be used to assess low, middle, and high frequencies3.
A similar advantage may be attained with the auditory steady-state response (ASSR), in which continuous, amplitude and/or frequency modulated tones evoke electrophysiologic responses that make possible a detailed and objective evaluation of hearing4.
Many researchers in this area have become interested in ASSR and tone burst ABR testing; these are promising tests, about which there is no consensus as to which is the best and fastest for clinical use. Existing studies have been made in adults; the Brazilian literature is particularly poor in describing these tests in term and preterm infants.
Thus, the purpose of this study was to investigate the clinical applicability of tone burst ABR and 2 kHz ASSR in infants by evaluating the time required for each test and comparing the responses of term and preterm infants.
MATERIAL AND METHODA cross-sectional, clinical, and experimental study was carried out at the clinic of the Speech Therapy School. The institutional review board of the university approved this study (process no. 0713/07). Parents and caretakers authorized the children to participate and the results to be divulged by signing a free informed consent form.
The inclusion criteria were: preterm or term infants, with normal meatoscopy in both ears, bilaterally present transient evoked otoacoustic emissions, presence of the cochlear-palpebral reflex at 100 dBSPL, and click stimulus BAPE within normal limits for each child's age. Absence of one or more of these criteria excluded of the subject from this study. A Welch Allyn Pocket Junior otoscope was used for performing meatoscopy, and a Smart EP (Intelligent Hearing Systems) device was used for OAE and click stimulus BAPE. The cochlear-palpebral reflex was investigated using an agogo. Thus, middle ear conditions, poor outer ear cell function, and neural/central hearing loss were excluded.
A statistics professional defined the minimum sample number at 30 subjects. Initially, 68 infants were selected for the study from October 2007 to July 2008. Twenty-three subjects were excluded by not meeting one or more of the inclusion criteria; testing was not concluded in a single session in nine subjects, who did not return to complete the tests.
Thus, the sample comprised 36 infants that were allocated into two groups according to the gestational age. The preterm group (gestational age < 37 weeks) comprised 17 infants (12 female and 5 male). The term group (gestational age from 37 to 41 weeks) comprised 19 infants (8 female and 11 male).
The Smart EP device was also used in tone burst ABR and ASSR testing. Before testing the skin was prepared with Nuprep (an abrasive paste). ECG conductive adhesive Medi-Trace electrodes (Kendall) were placed so that recording was ipsilateral to the stimulated ear; the impedance was < 5 kΩ. The electrodes were placed as follows: active electrode on Fpz, reference electrode on M1 or M2, ground electrode on the contralateral mastoid to the stimulated ear. Subjects remained sleeping naturally on their caretaker's lap during testing.
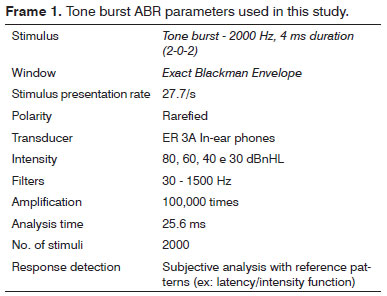
The order and ear for starting the test were random; tone burst ABR was done first on one infant, and ASSR was done first on the next infant, on the free ear depending on how each child was positioned on the lap of the caretaker. The test parameters were those of the manual and the pertinent literature (Frames 1 and 2). Because the two tests are time-consuming and were done during natural sleep, we chose to record a minimum electrophysiologic response at 2 kHz from each ear separately; the most reliable and lower thresholds are found at this frequency5.
This choice was also based on a pilot project with 10 infants that checked test feasibility relative to the number of frequencies and intensities that were studied.
In this pilot project, tone burst ABR and ASSR were recorded at 500, 1000, 2000, and 4000 Hz, and difficulties resulting from test duration (about 3 hours) were checked. This difficulty was still found when reducing the test to the frequencies 500 and 4000 Hz; we then decided for 2000 Hz, which was considered feasible to apply in a single session in the pilot project.
The chosen intensity was 20 dBSPL in the pilot projects, as most infants presented ASSR at this intensity; furthermore, the V wave (tone burst ABR) could not be identified accurately at 20 dBHL in any of the infants. This experiment helped define our test protocol.
The test duration was measured by two methods - a microcomputer clock and a KD-1069
® chronometer (Professional Quartz Timer). The former was used to measure absolute time (Δt abs) - the test duration from the beginning (after placing the electrodes) to the end (before removing the electrodes). Eventual pauses to control test conditions and/or the infant were also computed. The chronometer was used to measure relative time (Δt rel) - it was paused each time the test was stopped.
Rarefied stimuli were presented with ER 3A in-ear phones decreasingly at 80 dBnHL, 60 dBnHL, 40 dBnHL, and 30 dBnHL. The minimum electrophysiologic response at 2 kHz was measured by visual analysis of the V wave and reproducibility in two tracings.
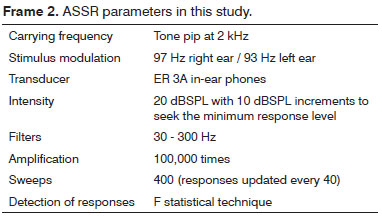
ASSR testing was started at 20 dBSPL with 10 dBSPL increments until obtaining the minimum response, since this was a hearing sample. ASSR testing was done with a maximum presentation number of 400 sweeps. If a response was attained with a smaller number of sweeps, the test was continued for two extra 40 sweep updates to check whether the responses persisted; this procedure avoided false positive results.
Fast Fourier transformation was applied to analyze frequency domain responses. The equipment detected the responses automatically based on F statistics, which assesses the response amplitude at the modulation frequency in relation to noise amplitude at adjacent frequencies. A response was considered positive if the signal-to-noise ratio was higher than 6.13 at a p-value below 0.05.
Descriptive statistics and non-parametric tests (Wilcoxon's test and Mann-Whitney's test) were applied in the analysis. Wilcoxon's test was applied to verify differences or similarities between left and right ears; the Mann-Whitney test was used for comparing the term and preterm groups. The significance level was 0.05 (5%); values without statistical significance were marked with an asterisk (*).
RESULTSThe study sample consisted of 55.6% females and 44.4% males. The mean gestational age in GT subjects was 39 1/7 weeks; at the evaluation, the mean chronological age of infants was 8 2/7 weeks. The mean gestational age in the GPT was 32 6/7 weeks; the post-conception mean age was 47 3/7 weeks. The analysis of both groups showed that there were no significant differences between right and left ears; thus, both ears were considered in the subsequent
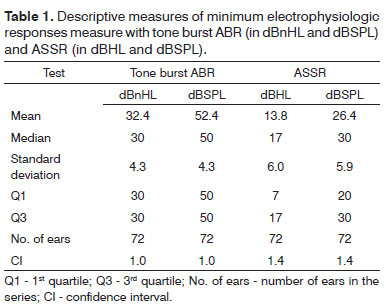
In 72 ears, the mean tone burst ABR minimum responses in nHL and SPL were 32.4 and 52.4 dB. The ASSR means in HL and SPL were 13.8 and 26.4 dB (Table 1).
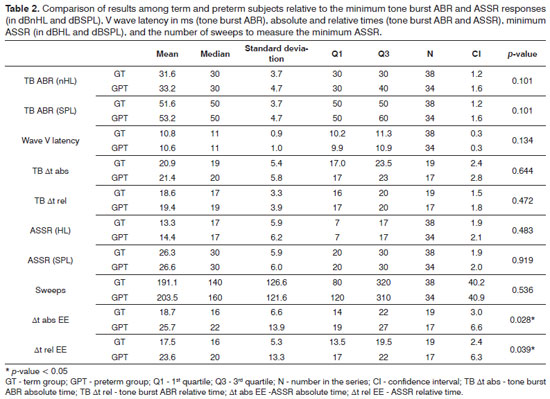
Comparing GT and GPT revealed no statistically significant differences except for the absolute and relative ASSR times; in this case, the GT had lower times for carrying out the procedures (Table 2).
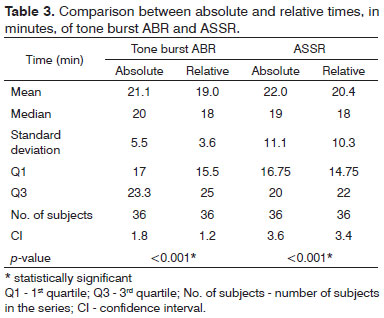
The absolute time was significantly higher than the relative time in test duration (Table 3), showing that pauses inevitably occur. The tone burst ABR mean times were 21.1 min (±5.5) and 19 min (±3.6). The mean duration of the ASSR was 22 min (±11.1), and the mean relative duration was 18 min (±10.3).
DISCUSSIONBefore starting the discussion, it is necessary to point out that comparisons between the tone burst ABR and ASSR is difficult to perform accurately, as there are differences in stimulus calibration (dBnHL for the tone burst ABR, and dBHL for the ASSR) and the response detection method in these procedures6. An additional issue is that most studies of these tests in children have been done with all subjects (or part of them) under sedation3,7-17. A few studies of infants in natural sleep and adults have chosen one of the ears randomly6,16,18-21 or by recording the responses in two channels22. These choices underline the difficulty of testing infants in natural sleep, especially when the intention is to perform tone burst ABR and ASSR testing in a single session.
Similarities in the side or ears - as noted in the present study - have also been reported in the literature7,23-25.
In the complete series (n = 72 ears) the mean minimum response was 32.4 dBnHL (52.4 dBSPL) at 2 kHz for tone burst ABR in the term and preterm groups. Studies with similar groups at the same frequency have reported lower results - in other words, better threholds7,16. However, these studies had different methods compared to our study: the minimum intensity was 10 dBnHL with two expert judges establishing the presence of the V wave,16 and stimuli at 2000 to 6000 were used7. A Brazilian study22 using 1500 Hz showed that 30 dBnHL may be considered a normal tone burst ABR intensity for infants and infants..
Analysis of the ASSR in our complete series showed that the mean minimum response was 13.8 dBHL (26.4 dBSPL) at 2 kHz. These data concur with other published results11,20,23,26.
Very few studies have compared thresholds measured with tone burst ABR and ASSR in the same population6,15,17,19,27.
The choice of two measurements of test duration was made to observe the true clinical application of these tools. Sedation for tone burst ABR and ASSR testing in infants is not a common practice in Brazil, as opposed to what occurs in other countires3,7,8,10-17; these tests in this country are usually performed by speech therapists in clinical settings. Relative time was equivalent to testing infants under sedation, that is, keeping ideal condition from beginning to end. Pauses were needed to maintain this condition and respect the infants physiological state as testing in this study was done with infants in natural sleep. Absolute time was the sum of the relative time and the pauses. Thus, absolute time was the true duration of testing with the chosen method. Absolute and relative times differed significantly in tone burst ABR and ASSR testing. Knowing this difference is important to define the testing protocols when reviewing other methods and comparing data.
Except for the duration of the ASSR, there were no statistically significant differences between the preterm and term groups in the comparative analysis. The literature contains some differences in comparisons of similar infants, in which preterm infants have worse thresholds, slower responses, and longer latencies compared to term infants20,22. However, these studies evaluated preterm infants with a mean post-conception age of 35 weeks, whereas this age was 47 weeks in our study. It is probable that maturation from the 35
th to the 47
th weeks was responsible for similar findings in preterm and term infants in the present study, which differs from previous work20,22.
Further studies of different population groups with other methods to study ASSR and tone burst ABR will help understand these techniques in greater detail to expand their clinical applicability.
CONCLUSIONThe results of this study led to the conclusion that the two methods - tone burst ABR and ASSR - may be applied clinically at 2 kHz in infants; the mean test duration was 20 minutes. Preterm infants require more time for ASSR, but in general showed no differences compared to term infants.
REFERENCES1. Gorga MP, Neely ST, Hoover BM, Dierking DM, Beauchaine KL, Manning C. Determining the upper limits of stimulation for auditory steady-state response measurements. Ear Hear. 2004;25(3):302-7.
2. American Academy of Pediatrics. Task force on newborn and infant hearing. Pediatrics. 1999;103(2):527-9.
3. Gorga MP, Johnson TA, Kaminski JR, Beauchaine KL, Garner CA, Neely ST. Using a combination of click- and tone burst- evoked auditory brain stem response measurements to estimate pure-tone thresholds. Ear Hear. 2006;27(1):60-74.
4. Lins OG, Picton TW, Boucher BL, Durieux-Smith A, Champagne SC, Moran LM, et al. Frequency specific audiometry using steady-state responses. Ear Hear. 1996;17(2):81-96.
5. John MS, Brown DK, Muir PJ, Picton TW. Recording auditory steady-state responses in young infants. Ear Hear. 2004;25(6):539-53.
6. Cone-Wesson B, Dowell RC, Tomlin D, Rance G, Ming WJ. The auditory steady-state response: comparisons with the auditory brainstem response. J Am Acad Audiol. 2002;13(4):173-87.
7. Chung YL, Tai HH, Shin LP, Chuan JH. Thresholds of tone burst auditory brainstem responses for infants and young children with normal hearing in Taiwan. J Formos Med Assoc. 2007;106(10):847-53.
8. Firszt JB, Gaggl W, Runge-Samuelson CL, Burg LS, Wackym A. Auditory sensitivity in children using the auditory steady-state response. Arch Otolaryngol Head Neck Surg. 2004;130(5):536-40.
9. Joong HA, Hyo SL, Young JK, Tae HY, Jong WC. Comparing pure-tone audiometry and auditory steady state response for the measurement of hearing loss. Otolaryngol Head Neck Surg. 2007;136(6):966-71.
10. Luts H, Desloovere C, Kumar A, Vandermeersch E, Wouters J. Objective assessment of frequency-specific hearing thresholds in babies. Int J Pediatr Otorhinolaryngol. 2004;68(7):915-26.
11. Luts H, Desloovere C, Wouters J. Clinical application of dichotic multiple-stimulus auditory steady-state responses in high-risk newborns and young children. Audiol Neurotol. 2006;11(1):24-37.
12. Hurley RM, Hurley A, Berlin CI. Development of low-frequency tone burst versus the click auditory brainstem response. J Am Acad Audiol. 2005;16(2):114-21.
13. Rance G, Dowell RC, Rickards FW, Beer DE, Clark GM. Steady-state evoked potential and behavioral hearing thresholds in a group of children with absent click-evoked auditory brain stem response. Ear Hear. 1998;19(1):48-61.
14. Rance G, Rickards FW, Cohen LT, De Vidi S, Clark GM. The automated prediction of hearing thresholds in sleeping subjects using auditory steady-state evoked potentials. Ear Hear. 1995;16(5):499-507.
15. Roberson JB Jr, O'Rourke C, Stidham KR. Auditory steady-state response testing in children: evaluation of a new technology. Otolaryngol Head Neck Surg. 2003;129(1):107-13.
16. Stapells DR, Gravel JS, Martin BA. Thresholds for auditory brain stem responses to tones in notched noise from infants and young children with normal hearing or sensorineural hearing loss. Ear Hear. 1995;16(4):361-71.
17. Stueve MP, O'Rourke C. Estimation of hearing loss in children: comparison of auditory steady-state response, auditory brainstem response, and behavioral test methods. Am J Audiol. 2003;12:125-36.
18. Rance G, Tomlin D. Maturation of auditory steady state responses in normal babies. Ear Hear. 2006;27(1):20-9.
19. Rance G, Tomlin D, Rickards FW. Comparison of auditory steady-state responses and tone-burst auditory brainstem responses in normal babies. Ear Hear. 2006;27(6):751-62.
20. Ribeiro FGSM. Estudo das respostas para o potencial evocado auditivo de estado estável em lactentes [tese]. São Paulo: Universidade de São Paulo; 2008.
21. Sininger YS, Abdala C, Cone-Wesson B. Auditory threshold sensitivity of the human neonate as measured by the auditory brainstem response. Hear Res. 1997;104(1-2):27-38.
22. Ribeiro FM, Carvallo RM. Tone-evoked ABR in full-term and preterm neonates with normal hearing. Am J Audiol. 2008;47(1):21-9.
23. Calil DB, Lewis DR, Fiorini AC. Achados dos potenciais evocados auditivos de estado estável em crianças ouvintes. Distúrb Comun. 2006;18(3):391-401.
24. Perez-Abalo MC, Savio G, Torres A, Martin V, Rodriguez E, Galan L. Steady state responses to multiple amplitude-modulated tones: optimized method to test frequency-specific thresholds in hearing-impaired children and normal-hearing subjects. Ear Hear. 2001;22(3):200-11.
25. Pinto FR, Matas CG. Comparação entre limiares de audibilidade e eletrofisiológico por estímulo tone burst. Braz J Otorhinolaryngol. 2007;73(4):513-22.
26. Souza EF. A utilização do potencial evocado auditivo de estado estável em recém-nascidos pré-termo [dissertação]. São Paulo: Universidade Federal de São Paulo; 2008.
27. Johnson TA, Brown CJ. Threshold prediction using the auditory steady-state response and the tone burst auditory brain stem response: a within-subject comparison. Ear Hear. 2005;26(6):559-76.
1. Master's degree in human communication disorders, UNIFESP. Speech therapist of the Medical Specialty Outpatient Unit (Ambulatório Médico de Especialidades or AME) São José dos Campos.
2. Doctoral degree in human communication disorders, UNIFESP. Associate professor, UNIFESP.
3. Doctoral degree in human communication disorders, UNIFESP. Adjunct professor I, UNIFESP.
Paulista Medical School (Escola Paulista de Medicina) São Paulo Federal University (Universidade Federal de São Paulo - EPM-UNIFESP).
Send correspondence to:
Maria Angélica de Almeida Porto
Rua Guarujá, 141, Jardim Apolo
São José dos Campos - SP. CEP: 12243-230
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on August 22, 2010
Accepted on October 24, 2010. cod. 7281
CAPES.