INTRODUCTION Benign necrotizing otitis externa is a rare affection, characterized by the onset of skin ulceration in the auditory external canal that deepens as a result of bone lysis, reaching the point of sequestration of tympanic bone. It is frequently mistaken by malignant otitis externa, neoplasia or cholesteatoma of the meatus and it is described as a peculiar characteristic of these diseases, that is, the authors do not realize that it is an independent affection. It is clinically similar to osteoradionecrosis, but patients do not refer history of local radiotherapy.
REVIEW OF LITERATUREAlso known as necrotizing osteitis, it was initially described by Goufas, in 1954¹. Although it is a well-known entity, it is frequently mistaken by malignant otitis externa 2, 5. It is normally manifested by non-painful chronic rhinorrhea, with ulceration of the floor of the external auditory canal, circumscribed by areas of bone necrosis. Its etiology is still unknown, and it is probably multifactorial, related to vascular abnormalities¹ or repetitive trauma of the external auditory canal³. Treatment is mainly clinical but it may occasionally be surgical 4.
CASE REPORTA S. M., Caucasian 84-year-old patient referred a manifestation of non-painful purulent secretion discharge through the external auditory canal on the left four months before, with no further otorhinolaryngological complaints. He did not refer diabetes mellitus, or previous radiotherapy or any other past otological affection.
At otorhinolaryngological exam, the patient presented facial paralysis and retroauricular hyperemia or pain upon palpation. In the external auditory canal we noticed a onecentimeter erosion on the posterior-superior region that communicated with the mastoid cavity, whose mucosa had normal aspect (Figure 1). There was no granulation tissue in the meatus, migration, retention of skin or bone sequestration. Tympanic membrane had normal anatomical characteristics. As a diagnostic attempt, we conducted supplementary exams that showed glycemia of 88mg%, bone scintigraphy (Gallium 67) with discreet captation and absence of growth of pathogen microorganisms in the culture of the external auditory canal. The biopsy of the border of the erosion revealed non-specific chronic inflammatory process, and temporal bone CT scan showed communication of external auditory canal and mastoid cavity that looked well aired (Figures 2 and 3).

Figure 1. One-cm erosion on the posterior-superior region that communicated with the mastoid cavity, whose mucosa had a normal aspect.
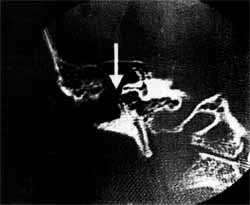
Figure 2. Communication of external acoustic meatus and a well aired mastoid cavity (arrow).
The otorrhea ceased with local treatment but discontinuity of meatus continued, but the patient returned to his hometown with no further complaints.
DISCUSSIONBenign necrotizing otitis externa, also known as benign necrotizing osteitis of the auditory external canal or meatus, is a pathology rarely described because it is normally mistaken by other external ear affections. It is a different clinical entity 4 whose etiology remains unknown, but it is probably related with repetitive traumas of the external auditory meatus 4, 5, such as the use of ear plugs3. It seems to be related to vascular abnormalities in the region¹, probably because of congenital alterations of the tympanic bone. We believe that some triggering factors, such as trauma, releases osteolytic cytokines in the, region that develop the necrotizing condition.

Figure 3. Communication of the external acoustic meatus and the mastoid cavity that seemed to be well-aired (arrow).
In the literature, there are no references to predominance of age, race or gender, although more male patients have been described, usually older than 50 years. The patients were not diabetics, nor had had any previous otological affection. They presented history of otorrhea, ranging from 1 to 6 months, associated or not with pruritus, otalgia and hearing loss 2,4,5.
As observed, our patient did not have characteristics that fit the most common external acoustic meatus diseases. His lesions seemed to be similar to those caused by radiotherapy (osteoradionecrosis), but the patient denied it: Other possibility was malignant necrotizing otitis externa, but the patient was not diabetic, the result of scintigraphy with Gallium 67 was discreet captation, and we did not notice grow of Pseudomonas aeruginosa or Staphylococcus aureus, the most common agents in this disease. Biopsy was negative for neoplasia and there was no migration of skin to the mastoid, both histologically and macroscopically. Based on that, we came up with the hypothesis of benign necrotizing otitis media.
Since there are few cases described in the literature, there is no consensus about the most adequate treatment. Sometimes, the use of topical drops of corticosteroids and aminoglycosides or dressings with both drugs, or even the use of acetic acid or boric acid, may lead to improvement of the case. Recently, surgical procedure was proposed requiring removal of the necrotic bone by curettage or using burs, and placement of temporal muscle fascia over the external acoustic meatus to promote reepithelization of the region 4.
Differential diagnosis should be made with malignant necrotizing otitis externa and with malignant neoplasia of the external auditory canal, besides osteoradionecrosis of the temporal bone and cholesteatoma of the external auditory canal.
Descriptions in the literature normally present cases of necrosis of the tympanic bone; however, our patient presenter the lesion on the region of the meatus that corresponds to the mastoid process.
Some authors confirmed the importance of having precise diagnosis of this disease in order to differentiate it from malignant necrotizing otitis externa 5, whose treatment is completely different, once previous history of radiotherapy would result in probable diagnosis of osteoradionecrosis and biopsy would confirm the presence of malignant neoplasia. In Chart 1 we see a comparison of the main clinical and investigation characteristics of benign necrotizing otitis externa and malignant necrotizing otitis externa.
Our patient was followed up for only some time because he had to return to his hometown. Talking with colleagues, we found out that they also had similar cases and that precise diagnosis was never made, because we tried to classify it into the common categories of diseases of the external acoustic meatus. Recent papers presented in congresses were also mistaken and presented all these characteristics with diagnosis of cholesteatoma of the external auditory meatus.
We believe that it is important to know this affection in order to promote appropriate study of the pathophysiology and future new treatment interventions.
FINAL COMMENTSBenign necrotizing otitis external is also known as benign necrotizing osteitis of the external acoustic canal, and it is a rarely described disease that affects mainly the tympanic bone. Its etiology remains unknown, and it seems to be related with repetitive trauma of the external auditory canal or vascular abnormalities of the region. We believe that total release of osteolytic cytokines is a triggering factor of the disease and studies addressing that topic should be conducted. The otorhinolaryngologist should know this affection and its clinical characteristics, which may be initially mistaken by other common diseases, such as malignant necrotizing otitis externa, malignant neoplasia of the external auditory meatus, cholesteatoma of the meatus and osteoradionecrosis.
CHART 1 - Comparison of clinical characteristics and investigation of benign necrotizing otitis externa (BNOE) and malignant necrotizing otitis externa (MNOE) - apud Wormald, 1994, modified.
*VHS: hemosedimentation rate
REFERENCES1. GOUFAS, G. - The diagnosis and pathogenesis of benign necrotic osteitis of the external meatus. Annals of Otolaryngol. (Paris), 71: 390-5, 1954.
2. KUMAR, B. N.; WALSH, R. M.; SINHA, A.; COURTENEYHARRIS, R. G.; CALIN, W. V. - Benign necrotizing osteitis of the external auditory meatus. The J. Laryngol. Otol., 111: 269-70, 1997.
3. RECK, R. & MIKA, H. Changes caused by ear moulds in the shape of the formation of the external auditory meatus. Laryngol. Rhinol. Otol. (Stuttgart), 57 668-72, 1978.
4. WORMALD, P J. - Surgical management of benign necrotizing otitis externa. TheJ. Laryngol. Otol., 108: 101-5, 1994
5. YOUNGS, R. & WILLAT, D. - Benign necrotizing osteitis of the external auditory meatus. The J. laryngol. Otol., 99. 05-8, 1985.
* Clinical Head of the Department of Otorhinolaryngology at Santa Casa de São Paulo and Joint Professor of Otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo.
** Assistant Professor of Otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo.
*** Resident Physician of the Department of Otorhinolaryngology at Santa Casa de São Paulo.
Study conducted at the Department of Otorhinolaryngology at Santa Casa de
São Paulo /SP
Address for correspondence: Rua Dr.Cesário Mora Junior, 112 - 01277-900
São Paulo /SP
Tel: (55 11) 222-8405.
Article submitted on February 24, 2000. Article accepted on August 10, 2000.
