INTRODUCTION Sulci, open cysts and iatrogenic lesions of vocal folds are characterized by adherence of mucosa in the vocal ligament, atrophy of mucosa and reduction of vibratory mass of vocal fold, and they are difficult to treat affections. Different techniques in therapy and phonosurgery have been described to help manage these patients. Phonotherapy is essential as a facilitator of vocal emission, either as an exclusive treatment or as part of the surgical intervention. Duprat et al. (1995) used vocal aggravation by relaxing the cricothyroid muscle (CT) and lowering the larynx, in order to augment the vibrating mass of the vocal fold facilitating its coaptation.
As to surgical treatment, a number of techniques have been described. Bouchayer et al. (1985) advocated incision of mucosa on the superior surface of the vocal folds, followed by detachment of adherence. Pontes and Behlau (1993) described detachment associated with stripping of mucosa, breaking lines of fibrosis. Isshiki et al. (1996) described framework laryngeal surgeries, type I thyroplasty, as an effective solution to correct glottic incompetence by atrophy. Techniques of injection and implants have gained space in our society to correct these affections by using synthetic or biological materials. Teflon was widely used at the beginning as an inert material; however, tissue reactions restricted its use (Nakayama et al. 1993), and fat and collagen injections are now more frequently used. Sataloff et al. (1997) later proposed the use of a bloc fat implant in the vocal fold, showing good results in cases of atrophy after laryngeal microsurgery. More recently, Tsunoda et al. (1999) started to use implant of autologous fascia to increase the volume of the atrophic area of the vocal folds.
Based on these studies, we proposed the use of autologous fat implants removed from the ear lobe in cases of sulcus, open cysts and post-surgical atrophies that did not present improvement with conservative treatment. The objective of the present study was to show our experience with the technique. We reported pre-surgical findings of 11 patients and compared the results after one and six months post-surgery using laryngeal videostroboscopy, vocal perceptual analysis and opinion of patient.
MATERIAL AND METHODTwenty-one patients were submitted to autologous fat implant in the sector of Laryngology of the Department of Otorhinolaryngology at Santa Casa de São Paulo, between March 1994 and March 1999. We selected patients that, had adherence of mucosa to the vocal ligament with affection of lamina propria, including patients with sulcus, open cysts and iatrogenic atrophy of vocal folds. Patients with closed cysts, vocal fold paralysis or fixation of arytenoids were excluded, as well as patients followed up before 6 months. All evaluated patients were being followed up by speech therapy when the surgery was indicated and they did not succeed with aggravation technique. Generally speaking, 11 patients underwent placement of fat by sulcus, open cysts and iatrogenic lesions caused by laryngeal microsurgery. Nine patients were female and two were male subjects. The mean age of patients was 32.9 years, ranging from 15 to 52 years.
CHART 1 - Relation of intra-operative diagnosis of 11 patients submitted to fat implant in Reinke's space.
Six patients had vocal folds sulcus, two bilateral and two associated with contralateral iatrogenic damage postlaryngeal microsurgery for removal of benign lesion. Four patients had open cysts, two of them bilateral. One patient had iatrogenic lesion post-laryngeal microsurgery for removal of benign lesion. Patients with bilateral lesions were approached on both sides at the same surgical time (Chart 1).
Surgery was conducted under general anesthesia. First, we performed the bloc removal of fat from the posterior face of the ear lobe, by making a l cm incision. The bloc had from 2 to 4mm in diameter, and it was maintained in a sterile solution of sodium chloride at 0.9% at room temperature during laryngeal approach. Using direct laryngoscopy with microscopy, a linear incision of the superior border of the vocal fold was made laterally to the affected region. Mucoligament adherence was detached, so that the size of the incision corresponded to two thirds of the extension of detachment, creating a pocket in the vocal fold to insert the graft. The block of fat was placed in the pocket, resulting in immediate increase in volume of the vocal fold. We tried to apply a larger amount of fat because of the partial absorption of the bloc.
Post-operatively, patients received intramuscular corticosteroids (10 mg of betamethasone dipropionate and 4 mg of disodium phosphate of betamethasone) and PO amoxicillin for one week (500mg TID We asked for relative vocal rest, avoiding whispered voice and vocal abuse. All patients started vocal therapy one week after surgery. Analysis of results was made by 1) vocal perceptual analysis, evaluating breathiness, harshness and voice breaks; 2) laryngeal videostroboscopy, defining vocal fold coaptation and characteristics of mucosal wave; and 3) opinion of patients about their vocal quality (worsening, maintenance or improvement) and sensation of vocal effort.
Patients were examined pre-operatively, and after one and six months post-operatively.
RESULTSIn the pre-op evaluation, the vocal perceptual analysis revealed breathiness in 10 patients (90.9%), being mild in four patients (36.36%) and moderate in the others (54.54%). Harshness was observed in all subjects (100%), seven of them moderate (63.63%), and four mild (36.36%). Voice breaks were identified in seven patients (63.63%) (Graph 1).
Laryngeal videostroboscopy showed spindle chink in 5 patients; middle posterior triangular chunk in two, hourglass chink in two, parallel chink in one, and posterior triangular chink in one case. Seven patients had interference of structural lesion in the mucosa wave (63.63%). All patients were unsatisfied with their voices, both because of its vocal quality and the effort necessary to produce it.
In the pre-op month, in the vocal perceptual analysis we noticed breathiness in 9 patients (81.81%), being mild in eight cases (72.72%) and moderate in one case (0.09%).'Harshness was present in 10 subjects (90.90%), mild in eight (72.72%) and moderate in two cases (18.18%). Four subjects (36.36%) had voice breaks (Graph 1). Laryngeal videostroboscopy showed spindle chink in 5 patients and effective coaptation during phonation. The other patients had middle posterior triangular, hourglass. and posterior triangular chinks. As to vibration of vocal folds, 5 patients (45.45%) had stiffness in the manipulated region, interfering with the mucosal wave. Eight patients (72.72%) referred improvement of vocal quality and three of them said it was a marked improvement (27.27%), with normal vocal pattern. Ten patients referred reduction of vocal fatigue and none of them reported worsening of vocal quality.
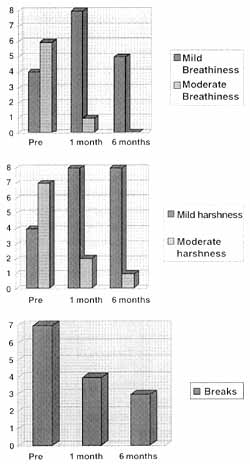
Figure 1. Pre-surgical, 1st, month and 6th month post-op perceptual analysis of voice. A) harshness, B) breathiness, C) voice breaks.
As to vocal perceptual analysis in the 6th post-op month, we observed breathiness in 5 patients (45.45%), being mild in all cases. Harshness was present in 9 subjects (81.81%), mild in 8 cases (72.72%) and moderate in one case (9.09%). Three subjects (27.27%) had voice breaks (Figure 1). Laryngeal videostroboscopy showed spindle chink in 3 patients and effective coaptation during phonation in 5 cases, 2 of them with middle posterior chink and one with hourglass chink. As to vocal fold vibration, 3 cases (27.27%) had stiffness where it had been manipulated, interfering with the mucosa wave. Eight patients referred improvement of vocal quality (72.72%) and 10 reported reduction of vocal fatigue. None of them reported worsening of vocal quality. Five patients (45.45%) reported effective improvement of vocal quality and normalization of phonation pattern.
DISCUSSIONApproach of patients with sulcus, open cysts and atrophies requires a joint action of the Otorhinolaryngologist and the speech and vocal pathologist. Patients started voice therapy about one week after surgery in order to improve quality of vocal fold vibration, glottic coaptation and to reduce vocal effort, besides correcting other phonation inadequacies that could have been associated. It has been observed that most of the patients with cysts, sulcus or scarring atrophies tend to increase the activity of cricothyroid (CT) muscle, stretching the vocal folds and making them thinner. Therefore, pitch becomes higher and glottic coaptation is less effective. In our service, we have used the technique of vocal aggravation, in which relaxation of CT muscle increases the mass of vocal folds and therefore improve coaptation and vibration. Half of the patients in our service have presented reduction of harshness, voice breaks and breathiness only with vocal therapy; we selected for the present study only those that had not improved with therapy (Duprat et al., 1995). Therefore, there is a number of patients that require surgical approach and this is the key topic of the present discussion. Vocal quality depends on integrity of the superficial layer of lamina propria (Reinke's space), a loose tissue with low viscosity, sliding its lamellae over the vocal ligament (Duprat 2001). The role of fat is to recreate Reinke's space, improving the sliding of mucosa over the vocal ligament and enabling good vibration during phonation. The fat would prevent new adherence of mucosa to the vocal ligament and increase the volume of the vocal fold, correcting common bowing and atrophy in such affections. The fat implant increases amplitude of vibration, phonation intensity and vocal efficiency and reduces phonation threshold (Wexler et al., 1989).
For the treatment of sulcus, Bouchayer et al. (1985) advocated incision of the mucosa on the superior surface of the vocal fold and later detachment of adherence; the mucosa is repositioned with biological glue. This technique does not allow for correction of volume and does not prevent a new adherence in the area. Pontes and Behlau (1993) proposed detachment followed by stripping of the mucosa to break the tension formed over the vocal fold; however, it does not preserve the integral mucosa. The technique proposed by our study not only preserves the mucosa, a determining factor for the success of phonosurgery (Bouchayer and Cornut, 198.5), but also enables correction of atrophy as it augments the volume of the vocal fold.
Atrophy and bowing prevents effective coaptation. Some techniques have been described to increase volume. Isshiki et al. (1996) described type I thyroplasty as an alternative, in order to medialize the atrophic area favoring coaptation of the vocal folds, and presented 31 cases submitted to this technique who presented improvement in vocal quality and reduction of vocal effort. However, in patients with atrophy caused by scar or sulcus vocalis, the results were not satisfactory. There was improvement of breathiness because of medialization of folds, but since the adherence persisted, the vibration remained impaired, with voice breaks and harshness, in addition to creating a vertical scar. In our opinion, techniques that enable the correction of adherence and volume simultaneously would potentially have better conditions to improve the vocal pattern.
The injection of materials such as Teflon was described in order to try to augment the volume and correct the atrophic area. Results were initially satisfactory but inflammatory processes, with formation of granuloma generated by the substance discouraged its use (Flint et al., 1997). The injection of bovine collagen was an alternative for small glottic insufficiencies. Ford et al. (1992) commented that a smaller absorption of collagen takes place when it is injected in the superficial layer - the smaller the chink, the better the results. However, since it is animal material, its employment face some limitations. The use of autologous materials, such as fat, has wide acceptance because it has low immunogenicity and mutagenicity, in addition to low cost. Brandenburg et al. (1992) described the injection of fat removed from the suction of abdominal wall, with good results in cases of scar and vocal fold paralysis, but no cases of sulcus or open cysts were described. Shaw et al. (1997) referred improvement of vocal pattern with injection of fat one year after surgery in patients with scarring atrophy; however, there was no improvement in the characteristics of the mucosal wave. In our cases, we observed improvement of mucosa wave. Preoperatively seven patients had stiffness, one month after surgery the number was five, and then 3 cases after six months. These data are similar to those reported by Sataloff et al. (1997), who showed improvement of vocal quality and mucosal wave in patients with atrophy.
The implant of bloc fat has shown better results than fat injection, suggesting that the bloc would have less reabsorption, when compared to the injection. The bloc implant
preserves the adipocytes integrally, and liposuction and injection may affect the fatty cells increasing the percentage of absorption (Sataloff et al., 1997). When attached, adipocytes release fatty acids generating a worse inflammatory process. The different approaches of fat implant justifies the different results found in the literature.
Figure 2. Mucoligament adherence corrected with fat showing the inflammatory process with collagen deposit. Fat prevents mucoligament re-adherence.

Figure 3. Mucoligament adherence corrected without fat. Collagen deposits creates bridges between the mucosa and the ligament resulting in mucoligament readherence.
Tsunoda et al. (1999) reported the case of temporal fascia implant in a patient with sulcus vocalis, presenting as satisfactory result in six months of follow-up and commented the advantages of the fascia instead of fat because it is a material less subject to reabsorption, providing long lasting results. Studies with more patients and experimental studies comparing both techniques will be important to define the best solution. Both procedures use autologous materials, but fat has viscoelastic characteristics closer to those of the superficial layer of lamina propria, and it may reconstruct more effectively Reinke's space (Chan a Titze, 1998).
Our findings show that after 6 months there was improvement of vocal pattern and improvement of the characteristics of the mucosal wave. Undoubtedly, there is partial reabsorption of fat and reduction of vocal fold volume. However, the bloc may interfere with the mucoligament readherence resulting in more uniform mucosa wave that provides better permanent results (Figures 3 and 4). Fat may restate the stability and periodicity of emission, in addition to reducing phonation threshold. Fat establishes symmetry and viscoelastic properties of the vocal fold (Jiang et al., 1994).
Of the 11 patients assessed, 10 of them (90.90%) reported improvement of vocal pattern and 5 of them (45.45%) referred normalization of pattern. Ten patients (90.90%) reported reduction of vocal fatigue. Breathiness was the vocal alteration that showed the best initial improvement: six (54.54%) had moderate breathiness and four (36.36%) had it mild. In the 6th month, only five (45.45%) had mild breathiness. Reduction of breathiness means that there is better coaptation, which associated with reduction of vocal fold stiffness, leads to reduction of vocal fatigue. Harshness went from moderate in seven cases (63.63%) and mild in four (36.36%) to moderate in one (9.09%) and mild in eight (72.72%). Reduction of harshness means reduction of friction between the vocal folds because there is more flexibility of vocal folds. Voice breaks were present in seven cases (63.63%) and went down to 4 cases (36.36%), showing less stiffness of the folds and' less interference with the mucosal wave. None of the patients presented worsening of vocal pattern after surgery, according to patients' opinion and vocal perceptual analysis.
Injection of fat is a safe technique; however, due to variable absorption, more studies are required to detect the factors that contribute to less absorption of implanted tissue, determining better results.
CONCLUSIONOur study showed that fat reconstructs Reinke's space forming a layer between the mucosa and vocal ligament, enabling more uniform vibration and reducing breaks and harshness. Upon increasing the volume of the atrophic area it is also possible to reduce breathiness. Therefore, fat implant is a safe and effective alternative for the correction of histostructural alterations of the vocal fold, and it should be considered as a therapeutic alternative in patients with atrophies, sulcus and open cysts.
REFERENCES1. ANDRADA, M. & COSTA, H. -,O exame da voz de cantores: um enfoque multiprofissional. Tópicos em fonoaudiologia 1995 in. Marquesan, I., Bolaffi, C., Gomes, L, Zorzi, J. Ed lovise 1995.
2. BOUCHAYER, M.; CORNUT, G.; LOIRE, R.; WITZIG, E.; ROCH, J. B.; BASTIAN, R. W. - Epidermoid cysts, sulci and mucosal bridge of the true vocal cord: a report of 157 cases. Laryngoscope 95: 1087-1094 - 1985.
3. BOUCHAYER, M. & CORNUT, G. - Instrumental Microscopy of Benign Lesion of the Vocal Fold. In: FORD, C. & BLESS, D., Phonosurgery, Assessment and surgical Management of Voice Disorders. New York, Raven Press, 1991. p.143-65.
4. BRANDENBURG, J. H. a col. - Vocal cord augmentation with autogenous fat. Laryngoscope; 102(5): 495-500, 1992.
5. CHAN, R. W. & TITZE, I. R. - Viscosities of implantable biomaterials in vocal fold augmentation surgery. Laryngoscope, 108: 725-31, 1998.
6. DUPRAT, A.; COSTA, H.; CAMPIOTTO, A.; ECKLEY, C. A terapia do agravamento vocal no tratamento do sulco vocal. Anais do 3° Congresso de laringologia a voz 1995 pg. 21.
7. DUPRAT, A. - Histoarquitetura e propriedades biomecânicas das pregas vocais. In: FERREIRA, L., P. & COSTA, H., C. Voz ativa. São Paulo, Roca. 2001, 113-26.
8. FORD, C.; BLESS, D.; LOFTUS, J. - Role of injectable collagen in the treatment of glottic insufficiency: a study of 119 patients. Anna Otol. Rhinol. Laryngol,, 101: 3237-47, 1992.
9. FORD, C. N. -Advances and Refinements in phonosurgery. Laryngoscope,109: 1891-900 - 1999.
10. FLINT, P.; CORIO, R.; CUMMINGS, C. - Comparison soft tissue response in rabbits following laryngeal implantation with hydroxyapatite, silicone rubber, and Teflon. Ann. Otol. Rhinol. Laryngol., 106 (5): 399-407, 1996.
11. ISSHIKI a col. - Vocal fold atrophy and its surgical treatment. Ann. Otol. Rhinol. Laringol., 105(3); 182-8, 1996.
12. JIANG, J.; TITZE, I.; WEXLER, D.; GRAY, S. - Fundamental frequency and amplitude perturbation in reconstructed canine vocal folds. Ann. Otol. Rhinol. Laryngol., 103: 145-148, 1994.
13. KASS, E. S. a col. - Vocal fold submucosal infusion technique in phonomicrosurgery. Ann. Otol, Rhinol. Laringol., 105(5); 341-7, 1996
14. NAKAYAMA, M.; FORD, C. N.; BLESS, D. M. - Teflon vocal fold augmentation: failures and management in 28 cases. Otolaryngol. Head Neck Surg. 96 493-8 - 1987.
15. PONTES, P. & BEHLAU, M. -Treatment of Sulcus vocalis: auditory perceptive and acoustic analysis of the slicing mucosa surgical technique. J. Voice, 7: 36-76 - 1993.
16. SATALOFF, R. T.; SPIEGEL, J. R.; Hawkshaw, M. Rosen, D. C.; Heuer, R. J. - Autologous Fat implantation for vocal fold scar: a preliminary report. J. Voice, 11: 238-246 - 1997.
17. SHAW, G.Y.; SZEWCZYK, M. A.; SEARLE, J.; WOODROOF, J. - Autologous fat injection into the vocal folds: technical consideration and long-term follow-up. Laryngoscope, 107: 177-186 - 1997.
18. TSUNODA, K.; TAKANOSAWA, M.; NIIMI, S. - Autologous transplantation of fascia into the vocal fold: new phonosurgical technique for glottal incompetence. Laryngoscope, 109: 504-508 - 1999.
19. WEXLER D., B.; GRAY, S.; JIANG, J.; TITZE, 1. Phonosurgical studies: fat-graft reconstruction of injured canine vocal cords. Ann. Otol. Rhinol. Laryngol., 98: 668-673, 1989.
* Instructor of the Department of otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo. Doctorate studies under course.
** Joint Professor of the Department of Otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo. Assistant Professor, Ph.D. of the program on Speech and Hearing Pathology at Pontifícia Universidade Católica de São Paulo.
*** Assistant Professor of the Department of Otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo. Doctorate studies under course.
**** Master dégree under course at the Department of Otorhinolaryngology at Faculdade de Ciências Médicas da Santa Casa de São Paulo.
Address for correspondence: Rua Professor Arthur Ramos 96, cjto. 72 - 01454-010 São Paulo /SP.
Article submitted on April 13 . 2000 . Article accepted on January 15, 2001.
