INTRODUCTIONDifferently from what we may expect, the term "sudden deafness" is many times used not to define a symptom, but rather to refer to a "one-symptom syndrome". It is due to the classification used by some French authors, such as Martin, H., 19783, who classified sudden hearing loss into two groups: an abrupt hearing loss (surdites d'apparition brutale), in which the etiology would be relatively clear, and sudden deafness (surdite brusque), of unknown etiology. This reasoning may lead professionals to identify symptoms as part of an idiopathic picture, especially when it is the sole symptom, defining management approach and discarding a more comprehensive investigation. We present here a case report of a patient who had a cerebellopontine angle tumor whose single symptom at diagnostic process was sudden deafness. We conducted a review of the literature and discussed the importance of a systemic investigation for better determination of etiology.
REVIEWIf we consider sudden deafness only as a symptom from different etiologies, we may classify its onset depending on the different pathophysiology of each situation. Zientalska, E., 199815, in his study, observed that 50% of sudden deafness events could be explained by vascular abnormalities; 25% by viral infections; 10% by traumatic episodes; 5% by allergic or autoimmune reasons, and only 10% were of unknown origin. It is surprising to observe that the author excluded cases of tumors of VIII nerve or adjacent areas but we believe that they were included in the vascular cases, since an explanation for the development of this symptom in the presence of a tumor would be the ischemia and consequent vascular compression caused by tumor growth. We know that in most cases of cerebellopontine angle tumors, the onset of deafness is progressive; however, authors such as Moffat, D. A., 19941, observed that about 10% of the cases of acoustic neuroma and 20% of the cases of vestibular Schwannoma progress showing sudden deafness. This high incidence is confirmed in the study by Fitzgerald, D. C., 19981, who observed some kind of significant morphological finding in 31% of the patients with sudden deafness submitted to magnetic resonance.
Another possible vascular etiology would include the pathologies that modify blood viscosity and vasculitis. Zheng, S., 199714 studied 14 different hemorrhage parameters of 50 patients with sudden deafness and observed that in 16% of the cases some factors were significantly altered, suggesting that abnormalities of blood viscosity and alteration of microcirculation are important etiological factors. In turn, Sun, A., 199711, found a significant incidence of anemia and other iron metabolism disorders (60.84%) in patients with sudden deafness. We should not forget about cases of vasculitis impairing vestibularcochlear system, such as in the case of Cogan syndrome, despite the fact that they are rare. Although embolic ischemia is frequently included as an etiological hypothesis in most literature reviews, this entity is rarely definitely diagnosed, as shown by Kim, J. S., 19992, when he had the rare opportunity of examining microscopically the temporal bone of a 92-yearold patient with recent sudden deafness, and he did not observe artery obstruction, but diffuse degeneration of the hearing system.
Viral etiologies are frequently suggested by authors, but they are also difficult to confirm, resulting in the classification of idiopathic causes. The significant number of studies, such as the ones by Ochi, K., 19987, which demonstrated a significant improvement in hearing with corticoid treatment suggested that viral etiology could be much more frequent than the number of cases really confirmed.
Currently, allergic and auto-immune etiologies are more frequently addressed by authors. Takahashi, M.,199812, studying 50 patients with sudden deafness classified as idiopathic, observed that 50% of them had immunological alterations, especially high titers of immunoglobulins.
Traumatic origin is not difficult to define as an etiology, but round window rupture, a fact many times referred as the possible explanation for the condition, is rarely confirmed.
Although today patients rarely simulate a sudden hearing loss because of sophistication of equipment and enhanced professional training, we should always be aware of cases of Muchhausen and malingers, who may compromise a correct diagnosis for some time.
Therefore, owing to the great number of possible explanations for the development of this symptom, as well as for the difficulties in confirming them, many cases are labeled as idiopathic, despite the fact that a somewhat more comprehensive investigation would produce objective data, leading to a more precise management of the case. If the diagnosis of idiopathic deafness is maintained, the physician is expected to suggesting a little invasive management that will somehow cover all the main problems that would result in the clinical picture. The literature reports the consensus about the use of corticoids, because of anti-inflammatory and anti-allergic effect, as well as vasodilators and hemorrheologic medications that bring some kind of improvement of plasma viscosity. Sano, H., 19989, reminded us of the significant improvement obtained when the treatment is started early, since it is much more time dependent than technical-dependent. Some authors, such as Zhang, X. Y., 199713, suggested alternative treatment options, such as the methods employed in traditional Chinese medicine, but the authors observed that in a comparative study between Eastern and Western methods, there was a more significant improvement with the latter, which does not prevent the traditional Chinese medicine to be used as complementary therapy.
CASE REPORTCaucasian female patient, M. L. B. L. R., aged 69 years old, without previous complaints involving ENT, presented with complaint of severe sudden hearing loss on the right ear for 5 days, without any other sign or symptom. She reported history of acute myocardial infarction followed by revascularization 5 years before. In the audiometry, she showed sensorineural hearing loss on the right ear, residual hearing levels close to 90 dB in all frequencies. The patient was immediately medicated with vasodilators (Cinarizine -150mg/day) and corticosteroids (Dexamethasone -18mg/day, in a regressive regimen), and we started etiological investigation. The patient had been regularly taking acetyl salicylic acid and the 500mg/day dose was maintained. Although the patient did not have any further complaints, we ordered magnetic resonance of temporal region, which showed a large infiltrate tumor mass on cerebellopontine angle, showing some cystic areas and leading to deviation of brainstem.
We also ordered Brainstem evoked potentials and otoneurological exams to gather a comprehensive academic documentation; however, after the diagnosis was made, the patient refused to be submitted to any further exams.
The patient was referred to the department of neurosurgery, but although she had been properly informed about the severity of the case and the possible management options, she has not authorized any invasive techniques so far (Figure 1).
DISCUSSIONSimilar to a case report presented by Merino, G. E., 19944, in which a patient with a cerebellar tumor had the sole symptom of sudden hearing loss, it was clearly stated in our case that regardless of starting the treatment, the idea of carrying on with the diagnostic investigation was fundamental, and without it, the case would be classified as idiopathic. Exams such as brainstem evoked potentials, skull base tomography and otoneurological exams should be part of any clinical analysis of sudden deafness, not only because of their high specificity, but also because they complement each other. Taking into account possible allergic, auto-immune or inflammatory etiologies, simple exams such as CBC and seric IgE dosages may emphasize clinical suspicions. Authors such as Michel, O., 19995, are great advocators of the need, whenever possible, of starting the investigation by performing magnetic resonance, together with the conduction of other exams, specially if the patient is hospitalized.
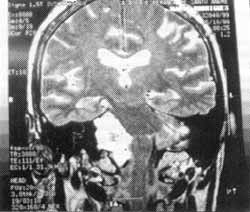
Figure 1. Magnetic resonance of patients showing a large tumor mass on cerebellopontine angle, deviating the brainstem.
Although traditionally the French school sets the theoretical base for academic Otorhinolaryngology in Brazil, understanding sudden deafness (surdite brusque) as a nosological entity seems to be more appropriate to Anglo-Saxon authors such as Schiff, M. and Brown, M., 197410, who face sudden deafness as a symptom and insist on the importance of conducting a systemic investigation for the etiological factor. This approach does not prevent the treatment from starting, especially regarding little invasive management options that aim at improving blood support or an inflammatory process; however, we should not resign ourselves to the simplistic diagnosis of idiopathic pathology.
REFERENCES1. FITZGERALD, D. C.; MARK, A. S. - Sudden hearing loss: frequency of abnormal finding on contrast-enhanced MRI studies. AJNR Am. J. Neuroradiol.; 19(8):1433-6, 1995.
2. KIN, J. S.; LOPEZ, I.; DIPATRE, P. L.; LIU F.; ISHIYAMA, A.; BALOH, R. W. - Internal auditory artery infarction: clinicopathologic correlation. Neurology; 52(1):40-4,1999.
3. MARTIN, C. H.; PIGNAL, J. L.; MARTIN, H. - Sur les surdites brusques. Apropos de 100 cas. C. Rend. Soc. Frang. Otorhinolaryngol. Pathol cervico-fac. Arnette.; edit, Paris, 1978, 341-51.
4. MERINO GALVEZ. E.; HELLIN MESEGUER. D.; GARCIA ORTEGA, F.; MONEJAR, J. M. - Sudden deafness and cerebellar tumor. J. Laryngol. Otol.; 108(7): 584-6, 1994.
5. MICHEL, O. - Magnetic resonance spectroscopy in sudden deafness. As early as necessary-as late as possible. HNO; 47(2): 73-5, 1999.
6. MOFFAT, D. A.; BAGULEY, D. M.; VON BLUMENTHAL, H.; IRVING, R. M.; HARDY, D. G. - Sudden deafness in vestibular Schwannoma. J. Laryngol. OWL; 108(2): 116-9, 1994.
7. OCHI, K.; MITSUI, M.; WATANABE, S.; NAKASHIMA, H.; OHASHI, T.; KINOSHITA, H.; KENMOCHI, M.; KATO, I. - The effects of high-dose steroid therapy on sudden deafness. Nippon Jibiinkoka Gakkai Kaibo; 101(11): 1311-5, 1998
8. PERMAN, E. - "Sudden deafness" has not been classified as a side-effect. No compensation from the Drug Insurance Authority. Lakartidningen; 96(10):1208, 1999.
9. SANO, H.; OKAMOTO, M.; SHITARA, T.; HIRAYAMA, M. - What kind of patients are suitable for evaluating the therapeutic effect of sudden deafness? Am. J. Otol.; 19(5):57983, 1998.
10. SCHIFF, M.; BROWN, M. - Hormones and sudden deafness.
Laryngoscope; 84(11):1959-81.
11. SUN, A.; WANG, Z.; LI, J. -Disturbance of iron metabolism and sudden hearing loss: a prospective and retrospective survey. Lin Cbuang Erb Pi Yen Hou Ko Tsa Cbib; 11(6):243-5, 1997.
12. TAKAHASHI, M.; SAKATA, A.; UNNO, T.; HOKUNAN, K.; SHIGYO, H. - Immunological abnormalities in patients with etiology unknown sensorineural hearing loss. Nippon Jibiinkoka Gakkai Kaibo; 101(10):1260-5, 1998.
13. MANG, X. Y.; QIAN, X. M. -Clinical study of sudden deafness treated with method of integrated traditional Chinese and Western medicine. Chung Kuo Chung Hsi I Chieb Ho Tsa Chib; 17(5):283-5, 1997.
14. ZHENG, S.; JIANG, R.; FAN, M. - Hemorrheological disorders in patients with sudden deafness. Sheng Wu I Hsueh Kung Cheng Hsueb Tsa Chib; 14(1):11-4, 57, 1997.
15. ZIENTALSKA, E.; MOSZYNSKI, B.; KAPISZEWSKA, D.; CZARNOCKA, E.; KOWNACKA, E. - The results of sudden deafness treatment. Otolaryngol. Pol.; 52(6):707-12. 1998.
* Otorhinolaryngologist graduated from FMUSP. Post-Graduate studies under course at Faculdade de Medicina da Fundação ABC.
Affiliation: Hospital Maternidade Cristóvão da Gama - Santo André/SP.
Address for correspondence: Cecil C. Ramos - Rua Javaés, 70 - Vila Assunção - 09181-570 Santo André /SP - Tel: (55 11) 444-2457 - E-mail: cecill@zaz.com.br
Article submitted on December 6, 1999. Article accepted on Tune 9. 2000.
